Some time ago I would answered yes, this was the case but I have tended to change my views over time or perhaps refine them over time.
There is a view that the more a person has difficulty expressing aggression or anger then the likelihood of suicide increases as the anger gets turned in on self. In support of this such research is quoted

Horesh et al (1997)
“Anger correlated significantly with suicide risk. Higher anger contributed synergistically to the suicide risk.”
DiGiuseppe et al(2007)
“Increasing evidence indicates that aggressive behaviour may be related to suicidal ideation and attempts. Many adolescents report intense anger immediately prior to their suicidal gestures. In one study, a third of adolescents who completed suicide displayed anger as their predominant mood just prior to their deaths.”
“Prior to suicide attempts adolescents may engage in intense verbal attacks or display physical aggression towards objects or people”
DiGiuseppe et al(2007) also conclude that anger inward turned has a higher correlation to hopelessness in suicidal adolescents than anger outward turned. However the outward turned is also correlated as well.
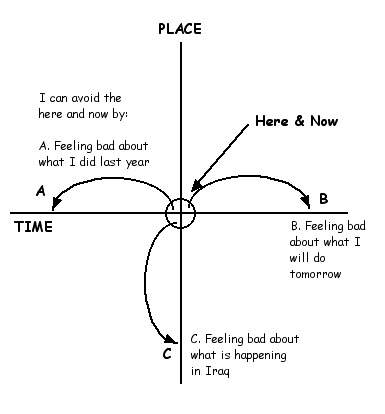
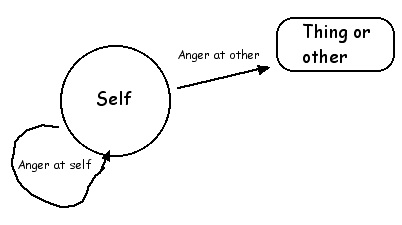
One firstly needs to identify the possibilities with anger
It seems reasonable to concur with the research. If a person has made the suicidal decision (“Don’t exist”) and they have high levels anger then they could be assessed as being at a higher risk of making some suicide action.
This would seem to be particularly so if the anger tends to be inward turned rather than expressed outwards as is shown in the diagram but I would also concur with the last conclusion of the research that there is also a correlation with outward turned anger as well.
When one sees a client who has inward turned anger one of the treatment directions is to get them to identify a thing or person to whom they could also direct some of the anger. The anger starts to be directed at something outside the person and thus one would assume that less of it is directed at the individual them self. This is a typical scenario in the treatment of depressed people.

However whilst the correlation was higher with inward directed anger there still was a correlation with outward directed anger. Getting the anger outward directed is better but still not the full solution. Why would this be so?
I have said before that psychologically there is some similarity between the murderer and the suicidal as well as some psychological similarity between the self harming person and the person who harms others. Some seem to find this hard to understand and take it as me saying that self harmers are in some way bad people for this. I am not saying such a thing and I have sought to find a metaphor that may make it clearer. I am not too sure if I have achieved this but I will give it a go anyway.

If I capable of speaking german then I can insult and verbally abuse others in that language. Or I can choose to insult and verbally abuse myself in german. If I have no mastery of the german language I do not have the choice. I cannot verbally abuse others in german and I can not insult myself in german. The self harmer and the “others” harmer both have mastery of the same language. They have both decided that physical assault is a viable solution to a problem. The person who does not harm self or others does not speak the language so they are far less likely to do either.
Thus we get back to the diagram and the research. Anger directed at self could obviously be correlated to suicidal behaviour. However anger directed out at others could also be correlated (but less so) because they are still speaking the same language than the person who does not have such anger in the first place.
In the treatment of such a kind of depression, one would first want the inward turned anger to start being directed at an outward thing or person. Once done then one would be wanting the person to drop the anger and thus they start to loose mastery of that language entirely.

Whilst on the topic of anger and suicide one can make further assessment of suicide risk by enquiring about how a person would plan to kill self. The method chosen could be reflective of the degree of anger involved. The more destructive the method may indicate a higher degree of anger involved.
The less violent methods would be things like poisoning self, gassing self or perhaps drowning and even cutting self in a effective manner (ie not hacking away at self). The more violent methods would include shooting self in the head, throwing self under a train or jumping from a high building. However it seems that the penultimate expression of violence in the act of suicide would be self immolation. Without a doubt a very violent means of suicide and reflective of substantial angry feelings.
Thus it seems productive for a therapist to enquire about the method of suicide considered and if violent then one knows to further look into the level of anger felt by the client and how they deal with such feelings.
One also needs to consider temper tantrum type of anger. If one sees a young child have a temper tantrum one would notice how they lash out in an indiscriminate way. Temper tantrum anger is completely directionless anger. The child is enraged and expresses that rage by lashing out at anyone including itself.
What is meant to happen in normal child development is slowly the child learns about its anger and learns to recognise the stimuli for the anger and then its anger expression is focussed at the identified cause. Some however never master this psychological task of child development and thus you get some adults who have the temper tantrum type expression of anger where its expression is indiscriminate. Hence you can have some suicidal type of behaviours when the tantrum anger gets directed at self.
In my view this can explain the situation where a 19 year old man goes into a school, starts shooting at people indiscriminately and eventually suicides at the end of it all. A temper tantrum type expression of anger.
If a client presents as having made a suicide attempt that seems to be anger related it would be instructive to question as to the context of that attempt. Namely, around the time of the attempt did the client display other indiscriminate anger expression. If he did then one may be dealing with an individual who has a temper tantrum type of anger expression and the suicidal behaviour is a consequence of that.

I am reminded of one person who almost completed a suicide in these circumstances. When I was working in a prison there was one inmate who had a phone call with his girlfriend where she dumped him and told him the relationship was finished. His response to this in the space of about 30 seconds was to smash the phone, slit his throat with a razor blade which he obviously had on him at the time and throw himself head first off a 4 meter high landing onto a concrete floor. The medical reports showed that he very nearly died, but he did survive. Indeed after that the other inmates referred to him as “Black magic” because he was black and it was magic that he did not die.
One could say that this suicide attempt was an angry act, but technically this is not correct. I got to know this man very well as that was my job in the prison, to identify and manage suicidal and self harming inmates. This man had not made the suicidal decision in childhood, he did not have a Don’t exist injunction.
What had happened was he was abandoned by his girlfriend to which he responded with rage. He then displayed that rage in a temper tantrum type of way. He damaged property (the phone) and then attacked himself (fortunately there was no one standing nearby or they may have been attacked as well).
His goal was not to kill himself, so technically it was not a suicide attempt, he was simply enraged and he expressed that anger in a temper tantrum where at one point he attacked him self. In such instances one gets the unplanned and spontaneous type of suicide attempts and thus many of them are not completed. In this case his anger was very reactive anger.
One can have other temper tantrum type of anger that is not reactive anger but is based on character anger. Thus an event does not happen that sparks the tantrum like anger but the person has character anger deep inside that pervades over time. In these circumstances one can get well planned suicidal and murderous acts. An example of this could be Martin Bryant.
He was an Australian in his early 20s. At one point he took a number of guns and considerable ammunition to a home where he shot dead two people he knew. After that he left and went to a popular tourist resort and randomly shot dead another 33 people. Any person, man woman or child who got in his sights he shot dead. At the sentencing the judge stated in part:
“The prisoner, having had a murderous plan in contemplation and active
preparation for some time, deliberately killed two persons against whom he held a
grudge, and then embarked on a trail of devastation which took the lives of a
further 33 other human beings who were total strangers to him and which caused
serious injury, distress and grief to literally thousands more. The repercussions
of these crimes have been world-wide. His selection of victims was
indiscriminate. He killed and injured men, women and even children”. (end quote)
After he killed the people at the tourist resort he left and went to a house where he set him self on fire in an attempt to kill himself. He survived the attempt and remains alive today.
Thus we have temper tantrum type behaviour. The indiscriminate killing of others and eventually the attempt to kill self. We have an instance of firstly controlled and thought out anger directed at a distinct target and then indiscriminate directionless anger expression.
Even in murder children will display a child like quality.
As another example
The Boomtown Rats were at a US radio station for an interview when the story
of Brenda Spencer came over the news wire. A 16 year old California high
school student made headlines when she grabbed her father's gun and opened fire
on her school from a house across the street, injuring eight students and killing
the school's principal and custodian. When later asked why she'd gone on the
shooting spree, she responded "I don't like Mondays."
I Don't Like Mondays
by the Boomtown Rats
“The silicon chip inside her head
Gets switched to overload.
And nobody's gonna go to school today,
She's going to make them stay at home.
And daddy doesn't understand it,
He always said she was as good as gold.
And he can see no reason
'Cause there are no reasons
What reason do you need to be shown?
Tell me why?
I don't like Mondays”.
Hence we have apparently unexplainable behaviour which mystifies many. The temper tantrum explanation may give some insight into why such things do occur.
Graffiti