Sara says:
“I do want to hear what self-soothing means not as a bunch of activities, but on a more basic level.”(end quote)
You are right, self soothing in the way I am using the term is related to attachment theory. Yes one can soothe self by having a bath or with music or with some other pleasant experience. That would be included with what I am saying but only be 10% of it
The soothing I am talking about is much more intertwined with relationship, security, and the soother must be content as well. The soother can’t fake it. The look on mother’s face in this picture is just as important as the child’s because soothing in this context is a relational experience for both parties. The child experiences its own soothing and it also experiences mother feeling soothed as well by it. Which of course is even more soothing for the child!

If this happens many times the child of course incorporates this and introjects it into its own Parent ego state. If as an adult it is feeling anxiety or depression it can then call on the sensory and somatic experience of feeling soothed but it also recalls mothers face as being happy and soothed by it as well and hence has a relational experience or understanding of soothing. Obviously a warm bath, or pleasant music can’t provide such relational experiences.
The thing is however, is that it wears off. Say that child got good parenting and soothing from its parents and then at age 20 leaves home. It can then use those early life experiences to self soothe when it is feeling distressed. But its not enough. As adults we continue to need soothing relational contact to keep filling up the bucket. We need ongoing relational contact with others where we feel soothed and we see in the others face that they are feeling soothed by us as well. If we don’t get such relational contact in adulthood then the bucket runs dry I’m afraid.
However the type and degree of refills required in adulthood is different depending on early life experiences. For instance that baby in the picture is getting pre-verbal soothing experiences. If one never got these then the refills in the adulthood bucket are needed much more and have less soothing effect.
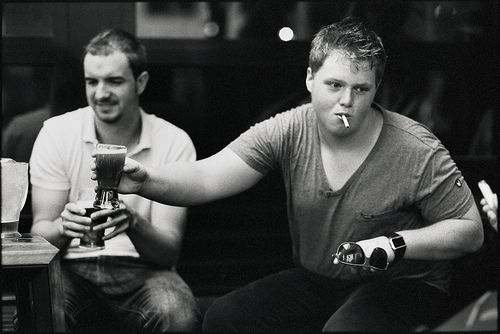
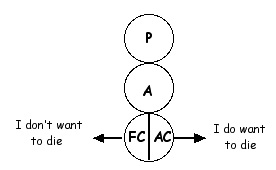
The self soothing of oral needs in adulthood.
But will it be enough?
The adult needs to some how get such pre-verbal soothing relational experiences. If she does then those fill up the bottom of the bucket and the subsequent adulthood refills are more effective in soothing the adult with unpleasant emotions.
However this raises an interesting notion. As I said before a mother soothing a child can’t fake it. If an adult person seeks a therapist to get some of these pre-verbal relational soothing experiences then the therapist cannot fake it!. So the therapist needs to have some sort of their own personal emotional investment in the client which the client can soothe in some form.
Thus one is left with a very fine line for the therapist to walk. The mother in the picture is using the child to meet her own emotional and relational needs just as much as the child is using the mother. Mother has needs and wants to ‘nest’, have babies, be a part of a family, be ‘clucky’ and nurture the infant. She has maternal instincts that she wants to be met. If she gets that then she feels her needs are met and is soothed herself. That is why she can’t fake it.

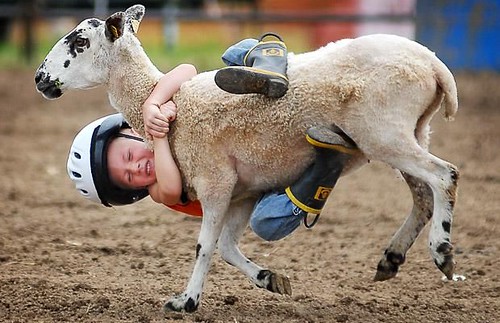
A child learning how to self soothe oral needs
A therapist has to be very careful about using a client to meet his or her own emotional needs and to use the client in such a self soothing way. However if the therapist views the client in a very clinical way and has no emotional investment in them then such relational soothing experiences will not happen for the client. The therapist can’t fake it. If a therapist is going to work with clients pre-verbal (or quite young child) issues then they have to walk the fine line just described.
On the other hand most people would get many of their adult fill ups from their partner. This is fine and is a good way to achieve such a thing. They can’t get their pre-verbal fill ups from their partner. If that begins to happen then your partner stops being your partner and starts becoming your therapist and that usually equals divorce at a later point.
Graffiti