Harriet states: I also thought of Carl Rogers when I read this. What did he say? Something like every person's goal should be to be the person who they truly are.
Carl said a lot of things Harriet. In his original writing there is a lot on transference that includes taped dialogue from sessions he did with clients. They are very interesting to read as one gets a bit of insight into how he worked as a therapist. However most of this is forgotten and he is most widely known for his clarification of the three essential features of the therapist in relationship with the client.
Genuiness - Therapist is aware of his own feelings, thoughts and attitudes and these are not concealed from the client.
Empathy - Understanding the client’s experience from the client’s point of view.
Unconditional positive regard - Conveying to the client that they are worthwhile humans no matter what they do.

Home wrecker
This has had a profound effect on the practice of psychotherapy which is why he is regarded as one of the greats of the field. As usual it is the simplicity that makes for it being more profound.
It seems reasonable to conclude that he was not the first to think this up. People would have known long before Rogers time that being genuine and empathetic was good for a relationship especially a helping relationship and I am sure teachers long before Rogers would have told their students such a thing. However he articulated it well and was in the right place at the right time and thus he became known as he is.
However this does raise an interesting and debated point of view. His approach and philosophy rests on the assumption that, “Love will cure it”. That is if you place a person into an environment or relationship that is genuine, empathetic and has unconditional positive regard they will naturally get better.

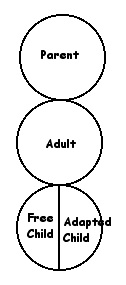
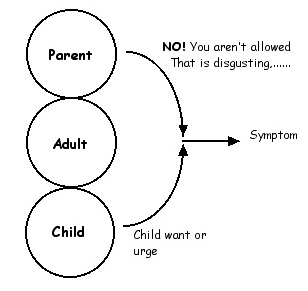
If you place a person in a nurturing and positive environment then their natural urge to grow and develop will be activated and the person will grow and develop towards psychological health. In transactional analysis terms it would be said that the Free Child aspect of the personality is energised or cathected and this is where the desire to grow towards health results from.
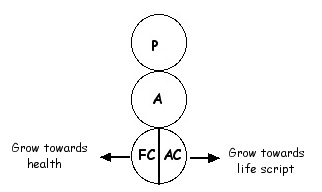
There is another school of thought that says, “Love alone is not enough for cure”. Without a doubt a loving, positive environment is good for one’s psychological health, but there is also an Adapted Child part of the personality that propels the person to ill health (or to their life script).
This side of the debate say that pure positivity is not enough to counter the drive to psychological ill health. At some point in the treatment you have to deal with this and that means doing something with the client that is experienced as painful in some way. That may be a confrontation of some kind that the client does not want to hear, getting the client to face their mother or father who abused them and so forth.
Some form of painful treatment is applied and this raises much heated debate. There are a group who say a client should never be subjected to painful treatment techniques with a common example being ECT or some form of aversion therapy like happened in the movie Clockwork Orange. You could argue that Carl Rogers would have been of the view that you do not apply painful treatments.
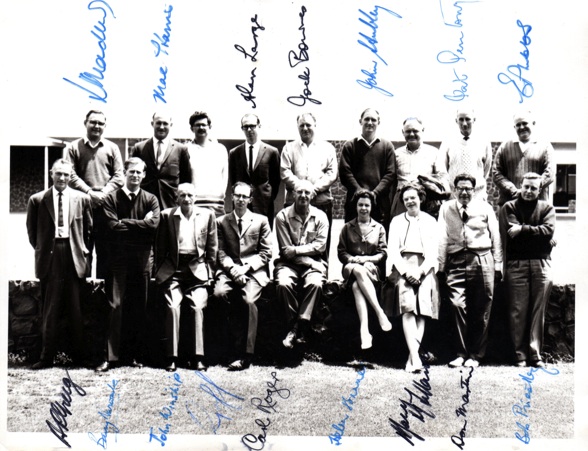
Carl Rogers workshop (1965)
My father back row third from right
Carl Rogers front and centre.
Of course there are much less dramatic painful techniques than ECT or aversion therapy and I certainly use some of them myself. For instance some two chair techniques could be placed in this category and this fits with my personal philosophy. Unconditional positive regard, empathy and genuiness as most useful in allowing the client to grow towards health but they are not enough in most instances. The AC is an active part of the personality that ‘love’ alone cannot over ride. It needs at some point to be dealt with directly and that usually involves some kind of angst for the client. Keep it to a minimum for sure but it is needed at times.
Graffiti