Here is the title and list of contents.

What they are doing to my book
Working with suicidal individuals: A guide to providing understanding, assessment and support
CONTENTS
PART 1. UNDERSTANDING SUICIDE
1. INTRODUCTION
The statistics
Goal of the book
The author's background
Terminology
The personal level for practitioners
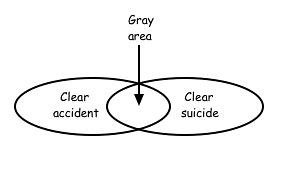
2. WHAT IS SUICIDE
What constitutes a suicide?
Accidents and suicide
Suicide by being killed
Conclusion
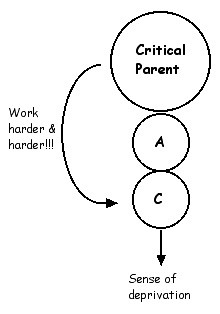
3. TRANSACTIONAL ANALYSIS
Theory of personality
Ego states and the newborn child
The functional ego states
Transactions
Conclusion
4. THE SUICIDE DECISION
Introduction
Decisions
The suicide decision
The process of early decision making
Aspects of the decision making process
Conclusion
5. MODELING SUICIDAL BEHAVIOR
Modeling and imitation
Modifying Parent ego state tapes
The suicide pact and supported suicide
Conclusion
6. REACTIONS TO HIGH STRESS
Regression
Three reactions to stress
Fight
Flight
Freeze
Suicide is usually a flight response
The counseling response to stress
Conclusion
7. SUICIDE AND SELF HARM
Self harm and suicide are separate
Bodily mutilation in context
The eight motives for self harming
Self harming with multiple motives
Harm minimization for the self harmer
Conclusion

PART 2. ASSESSING SUICIDE RISK
8. QUANTITATIVE MEASURES OF ASSESSING SUICIDE RISK
Alternate methods of assessing suicide risk
Suicidal thoughts
The quantitative approach
Accuracy of client information in reporting suicidal thoughts and behaviors
Quantitative measures
The tendency and degree of regression
History of high risk behavior
History of substance use
History of mental illness
Lack of any secondary gain
The prison population as a high risk group
Depression as an indicator of suicidal thoughts and actions
Single people are more likely to suicide than the married
Previous history of suicide attempts as an indicator of suicide risk
The suicide note as a measure of assessing suicide risk
Way of talking about suicide
Planning suicide as a method of risk assessment
Those with a flight response to stress
Conclusion
9. QUALITATIVE MEASURES OF ASSESSING SUICIDE RISK
Assessing long term suicide risk
Identifying the suicide decision
The Stopper Questionnaire
The Don’t exist interview
The bad day at black rock exercise
Reaction to the no suicide statement as a means of assessing suicide risk
Conclusion

PART 3. SUPPORTING THE SUICIDAL INDIVIDUAL
10. THE SUICIDE SECRET AND THE DELIBERATE SUICIDE RISK
Disclosing the suicide secret
The deliberate suicide risk
Conclusion
11. PSEUDO SUICIDE, SUICIDE AND TEENAGE SUICIDE
Introduction
The non suicidal
The suicidal - the suicide decision
The suicidal - command hallucinations
The suicidal - impulsive acts
Pseudo suicidal
Teenage suicide
Magical thinking about death
One teenager's statement about suicide
Another teenager's view of suicide
Conclusion
12. SUICIDAL AMBIVALENCE
Introduction
Understanding the ambivalence
Working with the suicidal ambivalence
Assessing the suicidal ambivalence
Conclusion
13. SUICIDAL TIMELINES
Suicidal behavior in context
The acute suicidal crisis
Slow developing suicidal crisis
Chronic suicidal crisis
Conclusion
14. THE NO SUICIDE CONTRACT
Origin of the no suicide contract
Theory behind the no suicide contract
Under the NSC iceberg waterline
The no suicide promise, no suicide assurance or no suicide commitment
The no suicide contracting procedure
To summarize the steps in the no suicide contract procedure
Refusal to make a no suicide contract
Conclusion
15. REDECISION THERAPY
The process of Redecision therapy
Contract for change
Diagnosis of early decision
Recreating the early scene
The redecision
Bring the client back to the here and now
Making behavioral contracts to carry out the new decision
Ongoing relational contact with the self destructive aspect of the client
Conclusion
Graffiti