See volume 2 here.
Graffiti
Showing posts with label suicide. Show all posts
Showing posts with label suicide. Show all posts
Sunday, December 29, 2013
Friday, October 11, 2013




Monday, August 26, 2013
How do suicide rates respond to elections
In Australia we have a federal election in two weeks.
A way to test the social integration theory of suicide posited by Durkheim in 1897. This theory suggests that the degree of social integration effects the propensity to commit suicide. Individuals who are only loosely connected to others in a society are at an increased risk of suicide. One way people display their attachment to a society is by participating in ceremonies that reflect common sentiments of the society. Every group of people has ceremonies that unite its members and expressed its shared ideals. These ceremonies foster greater integration by providing an opportunity for members to reaffirm their attachment.

Elections serve not only the functional role of assigning governance but also celebrates a mutual belief in liberty and self determination. Research in 1973 has shown that in the United States, in presidential election years there was statistically significant fewer number of suicides compared to the same months in non election years.
Other research in 1981 also found that suicides in election years were less than non election years. However it was also shown that both the percentage of suicide deaths and the percentage of all deaths were lower in election years.
This type of research supports the large body of research that shows during wars the suicide rate of a society tends to go down which some have said supports Durkheim’s theory of suicide.

This of course highlights the need for governments to have policies that enhance local social networks that exist and to develop new ways and types of social networking. After natural disasters encouraging families to move out of the area would seem to be contra-indicated.
Also raised is the area of networking through social media and can this have an impact on the degree of social integration experienced by people belonging to that network.
Graffiti
Friday, July 12, 2013
New book review - Working with suicidal individuals
Here is another book review I found from the journal, Mental Health Practice.
Also included is the latest list of university, college and training institutes that have the book. It is good to see such a wide variety have found the book to be an addition to their curriculum. Of particular note have been the additions in Europe most notably Poland, Norway, Sweden, another one in Slovenia, Ireland and the Netherlands. Also are a couple from South Africa and the first one from India.

Dublin Institute of Technology (Ireland)
National University of Ireland, Maynooth (Ireland)
Queen’s University, McClay Library Belfast (Ireland)
Queen’s University, Medical Library Belfast (Ireland)
University of Strathclyde (Scotland)
University of Stirling (Scotland)
Swansea University (Wales)
University of Glamorgan (Wales)
Bangor University (Wales)
University of Bergen (Norway)
Norges teknisk-naturvitenskapelige universitet (Norway)
University of Oslo (Norway)
University of Tromso (Norway)
Universitetet I Agder (Norway)
NLA Høgskolen (Norway)
Medical High School Juga Polak, Maribor (Slovenia)
Uniwersytet w Bialymstoku (Poland)
Nicholas Copernicus University (Poland)
Stockholm University (Sweden)
Högskolan Dalarna (Sweden)
Mid Sweden University (Sweden)
Hogskolan I Gavle-Sandviken (Sweden)
Swiss Federal Insitute of Technology Zurich (Switzerland)
Humboldt University of Berlin (Germany)
State and University Library of Dresden (Germany)
Bibliotheksservice - zentrum baden-württemberg (Germany)
Universitat Des Saarlandes (Germany)
University of Erlangen-Nuremberg (Germany)
Universitat Leipzig (Germany)
Bavarian State Library (Germany)
Stellenbosch University Library (South Africa)
University of Western Australia (Aust)
Murdoch University (Aust)
Edith Cowan University (Aust)
Bond University (Aust)
Monash University (Aust)
Australian National University: Online (Aust)
Victoria University (Aust)
Swinburne University of Technology (Aust)
Bankstown Campus library (Aust)
University of Sydney (Aust)
University of Adelaide (Aust)
University of Newcastle (Aust)
University of Melbourne (Aust)
University of Queensland (Aust)
University of Ballarat (Aust)
University of New England (Aust)
University of Western Sydney (Aust)
University of the Sunshine Coast (Aust)
TAFE Gosford campus library (Aust)
TAFE Bathurst campus library (Aust)
TAFE Tamworth campus library (Aust)
Deakin University (Aust)
LaTrobe University (Aust)
State library of Queensland (Aust)
Queensland University of Technology (Aust)
RMIT University (Aust)
Charles Sturt University (Aust)
MacQuarie University (Aust)
Australian Catholic University (Aust)
James Cook University (Aust)
National Library of Australia (Aust)
San Diego Christian College (USA)
Open Library. California State Library (USA)
University of Southern California (USA)
University of California San Francisco (USA)
University of California Merced (USA)
University of California Riverside (USA)
Loyola Marymount University California (USA)
Golden Gate University (USA)
California Institute of the Arts (USA)
California State University, Sacramento (USA)
MiraCosta College California (USA)
Carthage College (USA)
Beacon College Library (USA)
Freed Hardeman University (USA)
American University (USA)
Aurora University (USA)
Bay Path College (USA)
Kutztown University (USA)
Rogers State University (USA)
Mount Mercy University (USA)
North Central University (USA)
Plymouth State University (USA)
Philadelphia University (USA)
Davidson College (USA)
Daytona State College (USA)
DeSales University (USA)
Doane College (USA)
Fuller Theological Seminary (USA)
Simpson University (USA)
Union College (USA)
University of Saint Mary (USA)
Viterbo University (USA)
Biola University (USA)
University of Alaska - Fairbanks (USA)
Boise State University (USA)
Pepperdine University (USA)
Alverno College Library (USA)
Concordia University Technology Center (USA)
Graceland University (USA)
Lancaster Bible College (USA)
Lord Fairfax Community College (USA)
Seton Hall University (USA)
Wayne State College (USA)
Huntingdon College (USA)
University of Nebraska at Omaha (USA)
Catholic University of America (USA)
Gallaudet University (USA)
Virginia Tech (USA)
Old Dominion University (USA)
City University of Seattle (USA)
University of Washington (USA)
George Washington University (USA)
University of Miami (USA)
Miami Dade College (USA)
Georgia Southern University (USA)
University of Nevada - Reno (USA)
University of South Alabama (USA)
Iowa State University (USA)
Dordt College Iowa (USA)
University of Iowa (USA)
Training Library Ohio (USA)
Cornerstone University (USA)
College of Our Lady of the Elms (USA)
College of Western Idaho (USA)
Cameron University Oklahoma (USA)
Northwest Oklahoma State University (USA)
Butler Community College (USA)
Frostburg State University (USA)
Arizona State University (USA)
Arizona Western College (USA)
Brigham Young University Utah (USA)
Bloomsburg University (USA)
Massachusetts Institute of Technology (USA)
University of Massachusetts Amherst (USA)
Williams College Massachusetts (USA)
Hampshire College (USA)
Wellesley College (USA)
Boston College (USA)
Kean University (USA)
Keene State College (USA)
Cedar Crest College (USA)
Cedar Park Public Library (USA)
Colorado State University (USA)
Colorado Mountain College (USA)
Netlibrary Colorado (USA)
University of Colorado - Colorado Springs (USA)
University of Minnesota (USA)
Norwich University (USA)
Northwest Christian University (USA)
Santa Clara University (USA)
Stephen F. Austin State University (USA)
Saint Paul Technical College (USA)
Salish Kootenai College (USA)
Ithaca College (USA)
High Point University (USA)
Hamilton College (USA)
State University of New York - Plattsburg (USA)
University of Buffalo (USA)
Marquette University Raynor Memorial Library (USA)
Marian University (USA)
Millsaps College (USA)
City University of Seattle (USA)
National Library of Medicine Maryland (USA)
Illinois State University (USA)
College of DuPage Illinois (USA)
University of Chicago Illinois (USA)
Indiana University Bloomington (USA)
Central Michigan University (USA)
St Clair County Library (USA)
Crown College Library (USA)
University of Michigan (USA)
Grand Valley State University (USA)
Central Michigan University (USA)
University of North Carolina Chapel Hill (USA)
University of North Carolina Greensboro (USA)
University of North Carolina (USA)
University of Missouri-Columbia (USA)
University of Missouri-Kansas (USA)
Forrest Institute of Professional Psychology (USA)
Akron-Summit County Public Library, Ohio (USA)
Library of congress (USA)
Portland Community College Oregon (USA)
Mt. Hood Community College Library Oregon (USA)
National College of Natural Medicine Oregon (USA)
Oregon Health and Science University (USA)
Northeast WI Public Libraries (USA)
University of North Texas (USA)
Laredo Public Library Texas (USA)
Harris County Public Library Texas (USA)
Brazosport College Texas (USA)
University of Texas-Pan American (USA)
University of Texas at Dallas (USA)
University of Texas at Austin (USA)
University of Texas at San Antonio (USA)
Texas State University (USA)
St. Edwards University Texas (USA)
Texas Tech University (USA)
Lone Star College Texas (USA)
Dallas Theological Seminary (USA)
Sheffield Hallam University (UK)
Brunel University (UK)
Kingston University (UK)
Liverpool John Moores University (UK)
Loughborough University (UK)
Dept of Health, Isle of Man (UK)
Mersey Care NHS (UK)
Stowmarket library Suffolk (UK)
Northumbria University (UK)
King’s College London (UK)
Derbyshire library (UK)
Dorset County Libraries (UK)
Berrywood Library Northampton (UK)
Essex County Council eBook Catalogue (UK)
Oxford University library (UK)
Manchester Metropolitan University (UK)
University of Northumbria (UK)
Lancaster University (UK)
University of East London (UK)
University of Hull (UK)
University of Hertfordshire (UK)
University of Plymouth (UK)
University of the West of England (UK)
University of East Anglia (UK)
University of Cambridge (UK)
University of Exeter (UK)
University of Warwick (UK)
University of London, Goldsmiths (UK)
London Metropolitan Library (UK)
Coventry City Council library (UK)
The Berne Institute (UK)
The Link Centre (UK)
Bromley Library service (UK)
Cadbury Heath Library (UK)
Kingswood Library (UK)
Nottingham Central Library (UK)
Yate Library (UK)
Ipswich County Library (UK)
British Library, St. Pancras (UK)
British Library, Document supply (UK)
British Library, British National Bibliography (UK)
Ebook Library London (UK)
Hounslow Library (UK)
Barnet London Borough Library (UK)
Chipping Barnet Library (UK)
Hendon Library - Barnet (UK)
South Friern Library - Barnet (UK)
University of Manitoba (Canada)
Nova Scotia Community College (Canada)
Cape Breton University (Canada)
Memorial University of Newfoundland (Canada)
Grant MacEwan University (Canada)
University of Western Ontario (Canada)
Saint Francis Xavier University (Canada)
Saint Mary’s University (Canada)
University of Victoria (Canada)
Vancouver Island University (Canada)
Georgian College (Canada)
Ryerson University (Canada)
Royal Roads University (Canada)
Simon Frasier University (Canada)
St. Clair College (Canada)
University of Alberta (Canada)
Universite de Montreal (Canada)
Universite du Quebec (Canada)
Universite du Quebec en Outaouais (Canada)
Université du Québec en Abitibi-Témiscamingue (Canada)
Bibliotheques Universitaires du Quebec (Canada)
Memorial University (Canada)Memorial University - Newfoundland (Canada)
Mount Saint Vincent University (Canada)
Mount Royal University (Canada)
Wilfrid Laurier University (Canada)
Cambrian College (Canada)
Kwantlen Polytechnic University (Canada)
University of Lethbridge (Canada)
Dalhousie University (Canada)
Concordia University (Canada)
Concordia University College (Canada)
Grande Prairie Regional College (Canada)
Grande Prairie Regional College - Fairview (Canada)
Keyano College (Canada)
Olds College (Canada)
University of Guelph (Canada)
Library and Archives Canada (Canada)
Loyalist College (Canada)
Ngee Ann Polytechnic Library(Singapore)
Singapore Polytechnic Library (Singapore)
National University of Singapore (Singapore)
Nanyang Technological University (Singapore)
Hong Kong Academic Library (China)
Hong Kong PolyU Library (China)
Kaplan Business and Accountacy School (China)
National Chengchi University (Taiwan)
Taipei City Hospital library (Taiwan)
National Kaohsiung Normal University Library (Taiwan)
National Bibliographic Information Network (Taiwan)
University of Auckland Philson Library (New Zealand)
Mental Health Foundation of New Zealand (New Zealand)
Universal College of Learning (New Zealand)
University of Canterbury (New Zealand)
Lincoln University (New Zealand)
Northtec library (New Zealand)
International Pacific College (New Zealand)
Auckland University of Technology (New Zealand)
Unitec Institute of Technology (New Zealand)
Eastern Institute of Technology (New Zealand)
University of Otago (New Zealand)
Rotorua District Library (New Zealand)
Graffiti
Tuesday, February 19, 2013

Friday, February 8, 2013
Suicidality and normal adjustment - Part 2.
KYLady says
“This is an interesting post - the topic relates indirectly to my research. Behavior is influenced more by perceived risk as compared to actual (statistical) risk. Perceived risk can change day to day depending on events and conditions one is aware of. When risk becomes normal, people become more carefree about hazards they are exposed to. Normalized risk is a huge factor contributing to accidents on the job.” (end quote)
This is an interesting comment and adds to the concept of the normally adjusted suicidal person. It could be argued that a person can change actual risk to perceived risk simply by making the awareness of the danger unconscious. When that is the case the person will continue to act on their primary suicidal motivations even if they are not consciously aware of the behaviour they are using to express those motivations. Indeed this would put them at even greater risk of a completed suicide because of that lack of awareness.

If there is something that is clearly dangerous such as driving cars at very high speed and the person does not perceive it as dangerous they could have done that by making that information unconscious. They have employed some kind of defence mechanism to rationalize the risk away. This then makes the person at more risk of a completed “suicide” in the way I am talking about suicide in part 1.
A good example of this can be found in a case study in my book - Working with drug and alcohol users.
“A 37 year old woman recalls her thinking and feeling as she ignored harm minimization information.
"Never in wildest dreams did I EVER IMAGINE that I would share needles. Some of the details around these circumstances I can’t recall. I spose it was so traumatic, having a medical background and a deep moral code around sharing fits it still seems unbelievable.
I would ask the people who had used the fit before me if they had HIV or hepatitis and I chose to believe their response of no. Truth has no place in this world, if it shows up then is gets distorted, ignored or disproven because truth and drugs cannot be in the same room. The thought of not being able to get the drugs into me as quickly as possible especially when watching the others getting relief from their pain was something I could not take. This anxiety...fear far outweighs the fear for my own health and life. It was like trying to resist the sound of a newborn baby crying when you’re breast feeding.
I would disassociate from reality, time and space changed. I would wash the fit out with alcohol or bleech the whole time repeating a mantra of 'Please God, please God'. I would think who cares anyway, you’re fucked and life is fucked and you’re all fucked. Self loathing and the fear of not getting that rush would fuel me on.
Then the ritual of mixing up would begin and my mind would start bargaining “you’re not really going to do it” “you’ll stop before you whack it” but there is no stopping by this stage, you’re like a robot and this thing has you in its grasp. I would cry as I found a vein, wishing I could stop, jacking it back, holding in the sobs so I didn’t shake too much, then pushing it down the relief flooding over like a lover holding you in their arms no more 'aghhh!!' and once again I’m cleaver and funny, all worries dissolve, I am a sex goddess and philosopher, brave and complete, all fears drift away". (end quote)
This shows a number of defence mechanisms being used to make the danger unconscious. Or making the actual risk and perceived risk different.
Another quote from my book:
“1. Firstly she describes how she would ask others if they were carrying the HIV or hepatitis C virus. She knew the answer of ‘no’ could be considered quite unreliable. To proceed she must have used some mechanism like repression or denial to push the knowledge of unreliability out of her conscious.
2. Next she describes how she could dissociate which would allow her to decommission her Adult ego state temporarily which would allow her to proceed. This may have also assisted her discounting the unreliability of her peers reporting they were virus free.
3. Then she talks about repeating the mantra, “Please God please God”. This could be the defense mechanism of magical thinking where the Child ego state can feel safer because she has ‘prayed’ and this will some how magically make her safe.
4. Next she moves to an angry position with her comment, “I would think who cares anyway, you’re fucked and life is fucked and you’re all fucked.” This may be the defense of minimization. If she can convince herself that everything is bad then one little bit more of badness is not going to make any difference. It would allow her to minimize the importance of sharing needles.
5. Finally she talks about how her mind would start bargaining which may be a kind of rationalization. Convincing herself that her preparations for drug taking were not wrong because she will pull out at the last minute.” (end quote)

These five ways shows how she can perceive the risk to be less as the awareness of the danger becomes unconscious and she can continue to engage in the ‘suicidal’ behaviour which expresses one of the motivations in her personality.
Generally speaking people will not consistently behave in a particular way unless it reflects a basic part of their psyche or some primary motivation they have. They just will not do it for any length of time. If a person is not suicidal they will not do high risk behaviour even if the level of risk is unconscious. The unconscious will be reflected in repetitive behaviour just as the conscious will be.
Graffiti
Thursday, February 7, 2013
Suicidality and normal adjustment - Part 1
With the concept of passive suicidality one logically comes to define a different group of suicidal individuals. Most often suicidal people are seen to be despairing and desperate people who are enduring a great deal of suffering and pain. This group does exist and much has been said about them by a great many people.
Here is part of a model of human activity and level of risk. As one can see grand prix racing is one of the most highly dangerous activities one can engage in.
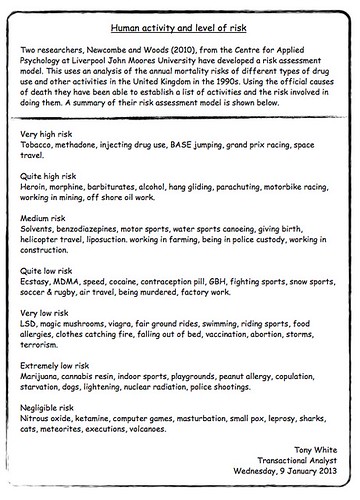
Those people who are such racing car drivers engage in this very high risk activity voluntarily, repetitively and over long periods of time. What does this say about those individuals? This must make some kind of statement about their psyche?
If someone engages in a piece of behaviour because they are pressured by others, or for a short period of time and then stops, or does it only occasionally then that says little about who they are and their psychology. But if someone does a piece of behaviour voluntarily, repeatedly and over an extended period of time then that says a lot about who they are and their internal psychological motivations. Humans will not do such ongoing repetitive behaviour unless it contributes to who they are and their life script. They simply wont do it for any length of time.
Such racing car drivers are knowingly and repeatedly putting them selves in a position where they know it may kill them. They are repeatedly placing self in a position where the risk of death is significantly increased. This speaks loudly about who they are and their internal psychological motivations and one could argue that this is suicidal behaviour. These people could be seen to be behaving in a suicidal way.

At the same time many of these people one could assume are reasonably well adjusted and certainly not like the usual suicidal person described above who is despairing and in a great deal of pain. Thus we are led to a position where one needs to reformulate the understanding of the suicidal person and indeed the concept of suicidality.
There is a group, indeed a significant sized group of people who engage in such suicidal behavior who are well adjusted and not suffering any significant depression, pain or angst. Suicidal behaviour is not solely restricted to the neurotic and maladjusted. It also resides in quite a sizable group of people who would generally be seen as psychologically well adjusted. Suicidality and normal psychological adjustment can exist in one individual at one time.
Two high profile Australian examples are Peter Brock and Steve Irwin. These two men died whilst engaging in high risk pursuits which they had been doing for many years. Indeed the high risk behaviour had become their occupations. Peter Brock died in a car accident whilst racing and Steve Irwin was making a film whilst swimming with sting rays. He died when he got to close to a sting ray and it shot its venomous 8 inch barb into him.
In this sense we have identified a new clinical group with quite different features from what is usually seen as the clinical status of the suicidal person. It is unusual because suicidality is generally considered quite an abnormal psychological state or it is seen to involve a significant level of maladjustment. However we have now identified a group who overall are generally well adjusted but still behave in an active suicidal way.

This amounts to an odd psychological situation. It is rare to find a person who is generally well adjusted but also has a specific piece of significant psychological abnormality. For instance most people whilst being suicidal also may have a mental illness, be a substance abuser, be depressed, have been in prison, be socially isolated and so forth. This is the usual clinical situation of the suicidal person.
We have now identified another group who do not fit this usual psychological profile. They repeatedly display suicidal behaviour but otherwise do not display any psychological abnormality.
Graffiti
Thursday, December 20, 2012
Terminating counselling with a client.
Introduction
When one employs a counsellor it is different to employing a plumber because you have to take the relationship into account as well. Indeed it is unique when compared to others in the ‘helping’ professions. When one goes to a doctor, surgeon, dentist or physiotherapist the relationship is clear. One goes for a specific goal and when that goal is achieved the relationship ends. Both parties know this from the beginning of the contact between them. Counselling is not like this. Firstly because the goals are usually less clear and the relationship between the client and counsellor is just as important (if not more important) than any treatment techniques applied.
Ending a relationship (attachment) is not an easy task. It does not matter what that relationship is be it siblings, spouses, friends and of course client and counsellor. It can be quite difficult for both parties no matter what the relationship.
Obligations between client and therapist
At this point it seems cogent to remember the underlying principles on which the relationship between the client and therapist are based. My thoughts are that the relationship is largely obligation free. (It should be noted that there would certainly be other counsellors who are of a different view on this matter). There is one out of four obligations required.
1. The client has no obligation to see a particular therapist
2. The therapist has no obligation to see a particular client
3. A client has no obligation to explain to a therapist why they wish to end therapy.
4. If the client requests it, a therapist has an obligation to explain to the client why they wish to end therapy.

The exit consultation
Sometimes a therapist will ask the client to contract to make an exit consultation. To agree to not just suddenly cancel an appointment or simply not show up and never contact the therapist again. They contract to make one final (exit) consultation should they choose to end therapy. The usual reasons for this are:
For a sense of completion of the gestalt for both the client and the therapist
To make sure the client is not leaving in a bad place
Counter transference and the exit consultation
These reasons seem reasonable and valid and if the client does agree to an exit consultation then this seems like a therapeutic thing to do. However there can be other motives why the therapist may make such a request and these can be due to counter transference issues in the therapist.
As mentioned before ending a relationship can be difficult and that is no different for a counsellor who may have developed some level of attachment to a client. It is hoped the counsellor would have some kind of supervision available should a difficult termination arise. The therapist may feel such thing like:
“I will use the exit consultation to try and talk the client out of it because I am insecure about my abilities and I take it as a personal rejection”.
The therapist may even be unaware they are feeling such things.
The counter transference termination transaction
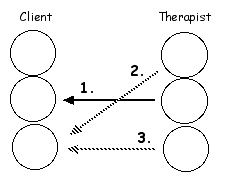
Transaction 1 is the overt Adult to Adult transaction that the therapist and client make with the exit consultation contract.
In conjunction with this the therapist can also have ulterior, covert and (probably) unconscious motives.
Transaction 2. The covert Parent to Child transaction: “Explain yourself”, “I don’t like ti when my influence is reduced”.
Transaction 3. The covert Child to Child transaction: “Please don’t reject me”, “Show me I am a good counsellor”.
Normal counter transference reactions
It seems safe to say that with some clients there will always be some kind of counter transference reaction when treatment ends. Especially if there has been quite a long period of treatment and if the therapist has developed some degree of psychological attachment to the client. When the relationship ends the therapist will have some level of a grief reaction. Hopefully the therapist is aware of this and may even communicate it to the client and then the termination can proceed relatively easily. The Free Child of the therapist will feel the pain of grief and bereavement in varying degrees.
Some therapists view this as a negative aspect of therapy and seek to avoid this normal counter transference by ‘keeping it clinical’. Some therapists become clinical in their view of the client and therapy and thus the attachment from the therapist to the client is kept to a minimum. The down side of this is you loose the therapeutic power of the client - therapist relationship. If the therapist is going to allow himself to develop some attachment to the client then one gains the advantages of the therapeutic relationship. However they also need to be aware of their tendency to get into their old self defeating relationship patterns that can interfere in the therapy process and make the outcome worse for the client.
Life script and terminating therapy
People tend to behave in patterns which means their relationships will tend to have patterns as well. In their relationships they will tend to do the same thing over and over again. The most important factor in the termination phase of counselling, is the client does not leave the therapeutic relationship in the same old self defeating relationship patterns. If this happens the client is using the ending of this relationship as a way to further their life script. They are ending the therapeutic relationship in a script bound way. It is most wise for the counsellor to raise this issue if they suspect it may be heading that way. Indeed some counsellors raise the issue with every client early on in the therapy.
For example if a client has a history of being rejected they may start to do a few things that will get the therapist angry or tired of them. They may start to not pay bills, they may consistently keep attacking the therapist personally, they may all of a sudden appear at the therapist’s home one night because they just have to see them then and there. It’s up to the therapist to identify and anticipate these relationship game maneuvers by the client so that the therapeutic relationship does not end up in the same old way for the client.

The No run contract
A “No run” contract is similar to an exit consultation but the reasons for it are different. The client contracts to make at least one more appointment before ending treatment. The motive behind it is that for some reason you want to lock the client into the therapeutic relationship. That may be to close the escape hatch of running from a relationship when the client feels reliance developing which may be their life script pattern. The counsellor is seeking to increase the clients distress by not allowing them to ‘run’ and then use those feelings in a therapeutic way. Or indeed it may heighten a sense of security for the client. There can be a whole range of motives for a therapist to suggest such a contract.
For the person who uses flight (compared to fight or freeze) as a basic coping mechanism such as the schizoid personality, it can be advantageous to introduce the idea of a no run contract quite early on, but it depends on how they do their flight. Some schizoids can 'flight' with physical relocation and hence the no run contract can be quite useful. Others don't have to move anywhere and will simply 'flight' in their mind and feel distance when they are sitting in the same room as the therapist. It is possible to have a psychological no run contract but that is harder to create and manage.

When the client terminates therapy without discussion
Sometimes a client will leave a message canceling an appointment and not making another one. Other times they simply do not turn up for the appointment and you do not hear from them again. The therapist is not given a chance to speak with the client when they terminate the therapy.
What therapists do in these circumstances varies greatly. Some will do nothing at all and others will actively pursue the client to talk with them directly. My own view is to take it on a case by case basis. Sometimes I do nothing and other times I will try and contact the client to speak with them.
This comes from CARMHA (2007) who are discussing working with suicidal clients.
“A client’s lack of follow-through with treatment may reflect hopelessness, pessimism, and cynicism regarding the value and benefit of treatment, and may be affected by the stigma of mental illness and suicide... Clients who reject help and withdraw prematurely from treatment tend to view interpersonal situations as risky and ripe for potential humiliation and emotional hurt”... (p10)
Speaking generically and not just about suicidal clients my view is that one needs to be careful not to harass or pressure a client. If that happens the client will either move into Conforming Child ego state and approach therapy from a conforming stand point which means the therapeutic process is significantly compromised. Or they shift into Rebellious Child and you never see them again.

This pressuring can happen particularly with the treatment of the suicidal where the therapist becomes a bit scared of a possible suicide attempt. This results in a change in the therapist’s behaviour such as how they deal with a client who drops out of therapy. The unusual behaviour of the therapist can result in outcomes one does not want. The therapist panics and ends up doing ‘poor’ quality therapy. When working with the suicidal one needs to often ask the question:
“If this client was not suicidal would I be doing what I am doing?”
Unlike the quote above I would suggest a significant number of clients stop attending because they are not ready to deal with what they are working with. Whenever I take a history of a new client I always ask if they have been been to counselling before and if they have, what happened and why did they stop. Not uncommonly they will say things like:
“I just was not in the right frame of mind.”
“I just wasn’t ready to do what was required at the time.”
“I had had enough by that time and needed a break.”
“I felt I was not getting what I wanted.”
I would say that rarely would a client report it was because they were afraid of interpersonal risk, because of stigma or because of the potential for humiliation. The examples I provide above I would say are much more common reasons.
Over the years I have had clients cancel appointments or just not turn up. Some I never see again and others come back later on. Indeed when a client ‘drops out’ that can be a used for therapeutic gain later on when they re-engage. One can use No run contracts, No engagement contracts, Phratry contracts and the like to create a variety of therapeutic scenarios for the gain of the client.
Graffiti
Reference:
Centre for Applied Research in Mental Health and Addiction. (CARMHA)
2007. “Working with the client who is suicidal : a tool for adult mental health and addiction services”. Simon Fraser University: British Columbia
Friday, December 14, 2012
Non attendance of sessions
This comes from a manual on the treatment of suicidal people. One can understand why they say what they say but one needs to be careful with it.

They also say

One needs to be careful not to harass or pressure a client. If that happens the client will either move into CC and approach therapy from a conforming stand point which means the therapeutic process is probably significantly compromised. Or they will shift into RC and you never see them again.
This pressuring can happen with the treatment of the suicidal where the therapist becomes a bit scared of a possible suicide attempt. This results in a change in the therapist’s behaviour such as how they deal with a client who drops out of therapy. The unusual behaviour of the therapist can result in outcomes one does not want. The therapist panics and ends up doing ‘poor’ quality therapy. When working with the suicidal one needs to often ask the question:
“If this client was not suicidal would I be doing what I am doing?”
How one deals with non attendance varies significantly depending on the client and the circumstances.
Some people, indeed I would suggest a significant number stop attending because they are not ready to deal with what they are dealing with. Whenever I take a history with a new client I always ask if they have been been to counselling before and if they have, what happened and why did they stop. Not uncommonly they will say things like:
“I just was not in the right frame of mind.”
“I just wasn’t ready to do what was required at the time.”
“I had had enough by that time and needed a break.”
“I felt I was just not getting what I wanted.”
I would say that rarely would a client report it was because they were afraid interpersonal risk, because of stigma or because of the potential for humiliation. The examples I provide above I would say are much more common reasons.

Over the years I have had clients cancel appointments or just not turn up. Some I never see again and others come back later on. Indeed when a client ‘drops out’ that can be a used for therapeutic gain later on when they ‘re-engage’ as they say in the therapy business. One can use No run contracts, No engagement contracts, Phratry contracts and the like to create a variety of therapeutic scenarios for the gain of the client.
However the most important point of all is that the client does not end therapy in such a way as to further their life script. They do not end the therapeutic relationship in a script bound way. It is most wise for the counsellor to raise this issue if they suspect it may be heading that way. Indeed some counsellors raise the issue with every client early on in the therapy.
Graffiti
Wednesday, October 31, 2012
Suicide spectrum disorder (revisited)
Wikipedia definition of spectrum disorder
A spectrum as it applies to mental disorder is a range of linked conditions, sometimes also extending to include singular symptoms and traits. The different elements of a spectrum either have a similar appearance or are thought to be caused by the same underlying mechanism. In either case, a spectrum approach is taken because there appears to be "not a unitary disorder but rather a syndrome composed of subgroups". The spectrum may represent a range of severity, comprising relatively "severe" mental disorders through to relatively "mild and nonclinical deficits."
Autism spectrum disorder

Substance use spectrum disorder

Suicide spectrum disorder

In suicide spectrum disorder at one end there are those situations where the death is clearly a suicidal act. At the other end there is behaviour that results in death which is clearly non suicidal, that is, clearly an accident.
To articulate the spectrum one has to isolate two aspects that relate to the act of suicide. In the suicidal individual there is
1. An experience of the urge or drive to engage in suicidal behaviour.
2. An ability to display behaviour that can result in a completed suicide.
It is hypothesized there is one group of individuals who have point 1 but not point 2 and another group who have point 2 but not point 1.
The ‘truly’ suicidal person has both point 1 and point 2. The ‘truly’ non suicidal person has neither point 1 nor point 2.

Hence we have our spectrum where there are two groups in the middle who if they die it is partly a suicide and partly an accident or the result of external actions or circumstances.
Suicide Spectrum Disorder
Case 1. Example of a person having (2. An ability to display behaviour that can result in a completed suicide.) and not having (1. An experience of the urge or drive to engage in suicidal behaviour.)
57 year old woman who has smoked cigarettes consistently since 17 years of age. She has given up once in that time for a two month period. In recent times she has been given medical advice that her lungs are starting to deteriorate significantly and should she continue to smoke she may have only about 5 years to live. Or at least in 5 years her physical health would be significantly compromised such that her standard of living is significantly reduced. The probability of her dying within the next 5 years is significant.
She states that she would like to give up smoking and in recent months has tried with in essence no reduction in her level of smoking. She is now of the view that should she die in her sixties that is OK. That it is quite a good life to have lived. To give up the pleasure she derives from smoking is simply not worth it.
This woman reports that she has never been suicidal, has never had any suicidal thoughts and has certainly never planned or attempted suicide.
This is a good example of a person who would fit in the accio-suicidal part of the Suicide Spectrum Disorder.
Case 2. Example of a person having (1. An experience of the urge or drive to engage in suicidal behaviour.) and not having (2. An ability to display behaviour that can result in a completed suicide.)
This is a case study presented in my book - Working with suicidal individuals.
A thirty year old man states he has had thoughts of suicide but says he could never actually do it. He has never made a suicide attempt. Instead he describes his reckless behavior as: "It's in the bad times when all the controls I have on myself I just let go of and it's, 'I will just do what I want'. This is when my drug taking becomes reckless. Also it's in those times when I can get full of drink, get in the car and go driving recklessly". When he is in this frame of mind the intravenous amphetamine use becomes reckless and there have been a number of hospitalizations due to over dose.
This man reports he simply can never imagine himself taking his own life. He can not imagine it in his behavioral repertoire. (end case study)
Another good example of the accio-suicidal part of the Suicide Spectrum Disorder.
In both cases the individual will not attempt to take their own life and hence will never die by what is usually seen as a suicide. Instead they will die by their own actions combined with external circumstances not in their control. Hence it is partly a suicide and partly an accident. It is a bit of both and hence we have a separate category on the suicide spectrum disorder.

In the first case example we have an interesting situation indeed. Here is a person who likes and enjoys her life and has no suicidal thoughts. In this way she could not be called suicidal at all. At the same time she is behaving consciously, consistently and over a long period of time in a way that is highly likely to cause her death. If she changed her conscious behaviour the likelihood of her dying is very significantly reduced.
One could argue she is suicidal and her suicidal urges are simply unconscious. Or one could argue this is not the case and is something else. If it is something else, what is it? Unfortunately at this juncture I do not have an answer to that question. I tend not to see it as unconscious because I know her very well and when one has unconscious urges they get expressed in some kind of way. I have not seen this happen with her, I know her history very well and have know her over a long period of time. If it is not hypothesized as unconscious then I have to be able to state what else it is and at the moment I cannot. I do not have the answer to that question.
Case two will be discussed further soon.
Graffiti
Subscribe to:
Posts (Atom)