See volume 4 here.
Graffiti
Tuesday, December 31, 2013
Sunday, December 29, 2013
Stroke deprivation
As Eric Berne said, “A stroke is a unit of attention” and one can have positive strokes and negative strokes. As a therapist it is easy to forget the importance of strokes and the important therapeutic role they can play.
The importance of them is no better demonstrated than by looking at a whole discipline or aspect of the science of psychology that is based on the psychology of strokes and that is behaviour modification.
Humans began to realize that how you respond to another person then influences how that person will think, feel and behave in the future. In behaviour modification terms you can respond to others with either positive reinforcement (strokes), negative reinforcement (strokes) or with no reinforcement (strokes) and that will influence how they behave in the future.
This remarkably simple discovery lead to the entire field of behaviour modification which has lead to probably millions of pieces of research on this very simple premise and has produced libraries full of books on the topic.
It is a huge area that is based on the premise, as I said, that how we respond to someone influences how they will behave in the future. Remarkably simple and yet remarkably powerful and of course the therapeutic implications are clearly evident.
If how I respond to a person can influence their future behaviour, this means as a therapist, I can respond to a client in a way which will influence how they behave in the future. Obviously a useful therapeutic approach to have.
Indeed this leads us to the basis of relational therapy. In therapy I will respond to a client with either a positive stroke, negative stroke, or no stroke. This then will influence their future behavior. The client will then respond back to me with either a positive stroke, negative stroke, or no stroke which in turn influences my future behaviour. The basis of relational therapy. It seems the psychotherapy of behaviour modification has been using a relational approach to therapy all along and it began in the 1950s.
Furthermore as the research on behaviour modification has shown you can’t avoid it. We are effected by the strokes we get from others. We can’t avoid being influenced by the strokes we get from others and often it is unconscious.
A most useful discovery so we set about refining the therapeutic applications of this discovery. In transactional analysis we discover that strokes can be conditional and unconditional and these effect the future behaviour of others in different ways. For instance with stroke power, negative strokes are more influential than positive strokes.
As negative strokes are more powerful then as therapists we should give clients Critical Parent negative strokes and that will help them to stop a behaviour like panic attacks. But it is not that simple. First the side effects of negative strokes damage the psychology of the person whereas positive stroke do not. Second, negative strokes may help a person to stop the neurotic behaviour in the short term but in the longer term it may actually get worse. As so often happens with human psychology, as soon as you start looking a bit deeper it gets more complicated.
But the basic premise remains. Sometimes we forget how important strokes are in therapy. People have different levels of stroke needs. Some require a lot day to day and others require less. However the important point is, when taking a client history how many of us ask about any level of stroke deprivation. From what I have seen not many. Are they getting enough strokes to meet their daily needs? If not, that is important as stroke deprivation can have a devastating effect on the personality.
An obvious example of this is depression. Some people are depressed because they are stroke deprived. Try this yourself. When you next have the chance spend as much of a day as you can getting no (or very few) strokes from others. You get no attention from others. Spend one day, two days, three days doing this and you will quickly discover how stroke deprivation leads to psychological collapse such as depression. Some people live in a state of stroke deprivation for years!
From what I have seen when a client presents with depression it would be uncommon for a therapist to look at stroke deprivation. Instead they start to look at internalized anger, high internal critic, changing internal self talk, history of depression in mother and father, potential suicidality, insomnia, eating problems, low self esteem and so forth?
In the DSM-5 the diagnostic criteria for major depression does not even mention stroke deprivation or psychological isolation. Hence my thesis that stroke deprivation is a significantly important aspect of psychological dysfunction and at the moment it is the forgotten relative and given little credence when the research clearly shows it is of significant psychological importance.
Of course therapy in itself is a big stroke. The client is getting a full hour of attention and can repeatedly do so on many occasions. If the client is reporting generally feeling better it could be partially due to the fact that the therapy is reducing their stroke deprivation.
One can use other techniques like the encounter exercise of stroke bombardment. To see that done is quite a moving experience and one again sees the value in simply reducing a person’s level of stroke deprivation which usually is not all that hard to do.
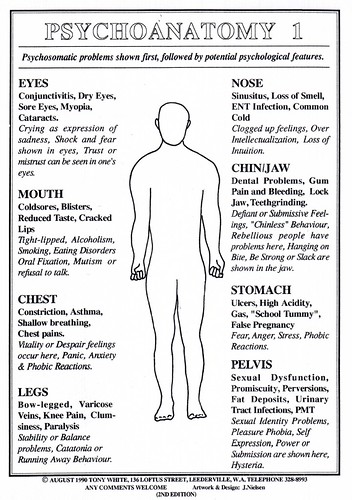
One can also separate strokes out into physical strokes and verbal strokes (both positive and negative)
Physical strokes have much more potency than verbal strokes. This chart would seem to suggest that to modify behaviour one would obviously use a negative physical stroke. If parents want a child to behave a particular way a negative physical stroke is most likely to achieve it. But as I said before the the problem with negative strokes (especially negative physical strokes) is they have unwanted side effects on the overall personality and they will also cause ruptures in the relationship between the parent and child. Positive strokes also modify behaviour and also produce side effects but these are wanted ones. But the unfortunate fact remains, negative strokes are more powerful in modifying human behaviour than positive strokes. This is why some parents use them - they work (at least in the short term). They get the short term result the parent wants.
With a stroke deprived person the best thing one can do is give positive physical strokes. But as we know professional organizations discourage therapists from touching their clients. So they actually cause the clients more problems. All therapists are left with is positive verbal strokes, which as we can see is the least powerful of all four.
Graffiti
Posters Volume 1.
In recent times (months) the format I have been writing in has changed. I have created a series of what I call information posters and been using them on my FaceBook. Over time these began to mount up so I began to collated them into volumes (three so far) which I have included here. I expect these to continue. Indeed I am in the middle of creating volume four right now.
See volume 1 here.
Graffiti
Thursday, November 14, 2013
Sunday, November 3, 2013
Drugs as a disease in society
This view one could say is widely held in the general population. Promoted mostly in the public arena by a variety of parties. The war on drugs approach typifies this view of drugs and alcohol in society. Indeed not uncommonly people will use terminology like 'disease' and ‘tearing at the fabric of society’ when talking about drugs and alcohol. Others will suggest that we are on the brink of a drug fueled crisis in society, especially with the youth of society.
The most recent being the alleged are, methamphetamine and crack cocaine epidemics occurring in society. Such prophecies come and go but there is generally speaking a new one occurring semi regularly.
Of course there is considerable evidence to the contrary and in the field of addictions counselling it is widely acknowledged that the vast majority of drug and alcohol users suffer very few, if any deleterious effects. It is only a quite small group who do.
A similar result is seen when one assesses the results of the stated drug epidemics. I am not aware of any society in the history of mankind that has been reduced to anarchy or has even been significantly negatively impacted by a drug problem. Plenty of societies have collapsed because of political problems, economic problems or religious disputes. These things are far more dangerous to society than mood altering drugs.

|
Problematic drug use
|
Prevalence
|
|
Cannabis use disorder
|
3.4% (12 - 17 year olds)
1.5% (18+ years)
|
|
Hallucinogen use disorder
|
0.5% (12 - 17 year olds)
0.1% (18+ years)
|
|
Inhalant use disorder
|
0.4% (12 - 17 year olds)
0.02% (18+ years)
|
|
Opioid use disorder
|
0.37% (18+ years)
|
|
Sedative use disorder
|
0.3% (12 - 17 year olds)
0.2% (18+ years)
|
|
Amphetamine use disorder
|
0.2% (12 - 17 year olds)
0.2% (18+ years)
|
|
Cocaine use disorder
|
0.2% (12 - 17 year olds)
0.3% (18+ years)
|
Tobacco has also been used for many hundreds of years probably originating in the Americas before being taken to Europe
Evidence has shown that opium was used in Mesopotamia at least seven thousand years ago
Archeologists in Northern Europe found remnants of cannabis dating back to the fifth century B.C.
Hallucinogenic drugs have also been very widely used throughout history dating back at least seven thousand five hundred years.

For a society to view itself as disease ridden is not a constructive thing. Indeed it could argued to be quite a deleterious thing for a society. Especially when what is seen as the disease is a psychologically normal thing for humans to do.
The 'war on drugs' and ‘drugs as a societal disease’ philosophy could be seen to significantly contribute to the view that we as a society have a disease or a bad bit in us. We are told this regularly in westernized societies. I wonder what it would be like if people started to see that drug use was not a disease in society. That it did not reflect a morally corrupt or dark bad bit in the cultural psyche. What would it feel like to feel good about ourselves in this way?
I know that in individual psychology for a person to stop seeing self as having a bad bit inside is a significant move forward with the corresponding increases in self respect and self esteem. If we as a society start doing the same would we as a society have the same positive results in our cultural psyches?
Graffiti
Graffiti
Saturday, October 19, 2013

Friday, October 18, 2013

Tuesday, October 15, 2013
Sunday, October 13, 2013



Friday, October 11, 2013




Tuesday, October 8, 2013
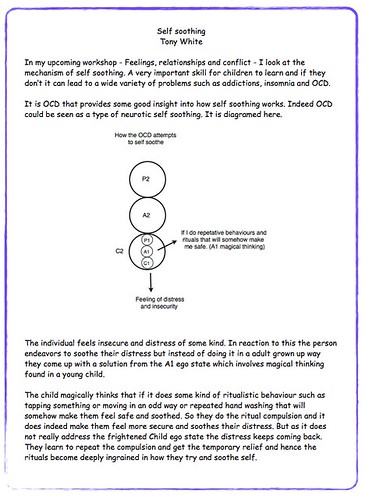
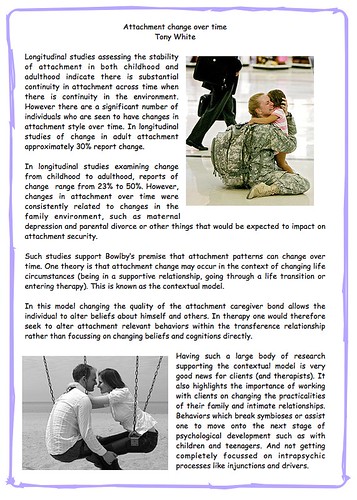
Attachment
In recent times I have been presenting my writing on FaceBook and working out a style by which to do that. What has evolved is a thing which I call posters which is a writing style that suits the FaceBook culture. But now the posters are mounting up and I don't know what to do with them so I decided to present them here in groups of related writings. I have done 4 on attachment.


Graffiti
Graffiti
Monday, August 26, 2013
How do suicide rates respond to elections
In Australia we have a federal election in two weeks.
A way to test the social integration theory of suicide posited by Durkheim in 1897. This theory suggests that the degree of social integration effects the propensity to commit suicide. Individuals who are only loosely connected to others in a society are at an increased risk of suicide. One way people display their attachment to a society is by participating in ceremonies that reflect common sentiments of the society. Every group of people has ceremonies that unite its members and expressed its shared ideals. These ceremonies foster greater integration by providing an opportunity for members to reaffirm their attachment.

Elections serve not only the functional role of assigning governance but also celebrates a mutual belief in liberty and self determination. Research in 1973 has shown that in the United States, in presidential election years there was statistically significant fewer number of suicides compared to the same months in non election years.
Other research in 1981 also found that suicides in election years were less than non election years. However it was also shown that both the percentage of suicide deaths and the percentage of all deaths were lower in election years.
This type of research supports the large body of research that shows during wars the suicide rate of a society tends to go down which some have said supports Durkheim’s theory of suicide.

This of course highlights the need for governments to have policies that enhance local social networks that exist and to develop new ways and types of social networking. After natural disasters encouraging families to move out of the area would seem to be contra-indicated.
Also raised is the area of networking through social media and can this have an impact on the degree of social integration experienced by people belonging to that network.
Graffiti
Saturday, August 24, 2013
Thursday, August 15, 2013
Gambling addiction vs drug addiction
The DSM-5 includes gambling addiction in the substance-related and addictive disorders along with the drug and alcohol addictions. Whilst this could be seen as a widely held belief that gambling should be included in such a category along with drugs and alcohol it does have some difficulties.
Firstly, in my book I see the dependent drug user as having an attachment problem and this get transferred onto the drug and the person develops an attachment to the drug in the same way they develop an attachment to mother or father.

The person forms a symbiosis with the drug where the drug takes over the Parent (and to a lesser extent Adult) ego state functions. Most obvious is the soothing effects of the Parent ego state. Dependent drug users are notoriously poor at self soothing. Drugs are very effective at soothing the drug user.
In normal development a young child uses mother's Nurturing Parent ego state to soothe itself and then it learns to self soothe as it grows. Dependent drug users don't learn to do this and hence needs an outside 'thing' to do it for them and hence the drug fills that role.
In gambling there is no where near the same soothing effect. At the very best there may be a kind of mild soothing effect in the act of gambling for some but compared to the soothing that heroin can provide it is next to nothing. Hence the gambling addict does not form a symbiosis with the act of gambling in the same way a drug addict develops a symbiosis with the drug. Thus we see one very crucial difference between the gambling addict and the drug addict and why it could be seen as erroneous to include them in the same category as the DSM-5 does.
I am not saying that a gambling addiction should not be seen as an addiction. What I am saying is that such an addiction is significantly psychologically different to an addiction to drugs or alcohol and it needs to be recognized as such. And as a result one cannot use the same treatment methods for a gambling addiction as they use for a drug addiction.
One could argue that a gambling addiction is really a passive behaviour. As we know the four passive behaviors are:
Doing nothing
Over adaptation
Agitation
Violence or incapacitation
I am now going to contradict myself in what I said in gambling addition 1. In that post I said gamblers do not seek to form a symbiosis with another in the same way a drug addict does. The drug addict seeks to use another's Nurturing Parent ego state to self soothe whereas the gambling addict does not as gambling does not have the same soothing effect that drugs do.
Having said that, I now say that a gambling addiction could be seen as a passive behaviour and as we know the purpose of a person behaving in such a passive way is to form a symbiosis with another person. In my hypothesis the gambling addict has a very strong drive to do such a thing but in a different way to the drug addict.
A gambling addiction could be seen as a form of incapacitation. The person gets them self into a position where they are incapacitated and then some one else of some organization comes along and looks after them.
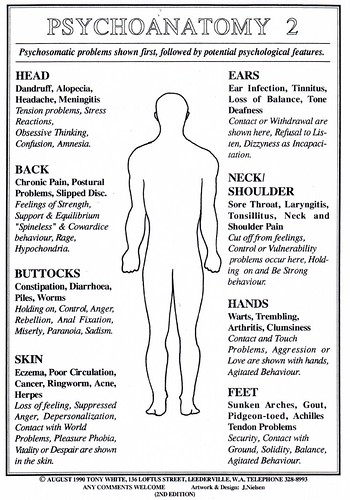
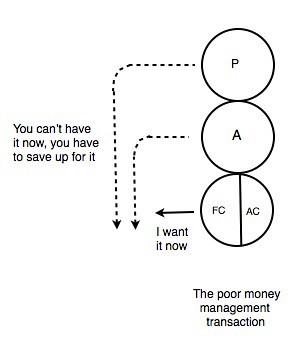
The gambling addict in essence does not manage money well. People who do not manage money well have an over active hedonistic Free Child that cannot be controlled by their Adult or Parent ego states.
As the transactional diagram shows the Parent and Adult are not strong enough to contain the Free Child want for the thing. I used this same diagram in my book to show how the recreational drug user functions. The recreational drug user can say to their own Free Child, “You have had enough now.” and the Free Child stops. The drug addict does not have that control over the Free Child. The same applies for the recreational gambler and the gambling addict. Indeed the same applies for any person who has high levels of credit card debt. They cannot control their Free Child want for the ‘thing’ now.

Graffiti
Friday, August 9, 2013
Collectivist couples counselling
In marital counselling the therapist needs to see a marriage as more than just two people

Graffiti
Graffiti
Thursday, August 8, 2013

Sunday, August 4, 2013
Wednesday, July 31, 2013
Book review - Working with drug and alcohol users.
This comes from the quarterly magazine of the United Kingdom Association for Transactional Analysis (Summer 2013)
The book review editor states:
The second book takes us to clinical work with alcohol and drug dependent clients. Tony White’s Working with Drug and Alcohol Users: A Guide to Providing Understanding, Assessment and Support was also published last year, by Jessica Kingsley. Tony White, a TSTA living and working in Australia, also wrote Working with Suicidal Individuals: A Guide to Providing Understanding, Assessment and Support, reviewed by Sue Brady in the Transactional Analyst (Autumn 2011). Jo Moores, TA psychotherapist and trauma specialist, gained experience of the complex world of substance dependency when working with The Big Issue In the North. Jo recommends Working with Drug and Alcohol Users as both ‘an accessible and concise introduction to our relationship with substances and the different roles they play in our lives’, and also as ‘a reflection of the author’s extensive experience and practice wisdom’. After an overview, Jo engages critically with Tony’s ‘TA theory of addiction’. She argues for the importance of the development of our theory on this central issue.
Readers are invited to write in with their views.
Dr Celia Simpson
Review
Working with Drug and Alcohol
Users: A guide to providing
understanding, assessment and
support.
By Tony White
Published by Jessica Kingsley
Publishers, London, 2012.
Review by JO MOORES
TONY WHITE’S BOOK brought back to me a vivid memory of working with people who were street homeless and who invariably had substantial drug and alcohol problems. The memory was of a young woman fresh from detox who was talking about how she could build a life for herself without drugs. She became deeply distressed and disclosed experiences of being raped. For her, life without the emotional blanket of heroin felt untenable as she was flooded with traumatic memories. A few days later I saw her back on the streets asking for money, eyes glazed over and, as Tony White would say, back in a symptomatic relationship with her drug of choice.
This book is an accessible and concise introduction to our relationship with substances and the different roles they play in our lives. Speaking in the same breath of cocktail parties and injecting heroin users, White destigmatises the very human act of using substances to alter our minds, moods and experiences. Working with Drug and Alcohol Users manages to be both a beginner’s guide to the complex world of substance dependency and a reflection of the author’s extensive experience and practice wisdom.
Part One is titled ‘The Foundations of Drug and Alcohol Counselling’ and contains useful information about different kinds of drugs, self disclosure, drug induced psychosis, gateway and poly-drug use and the different perspectives on addiction and treatment that have developed over the past century . In addition to providing the reader with a basic introduction to Transactional Analysis, Tony White then builds his case for the centrality of relationship and identity formation in the development of substance addiction, using the concepts of symbiosis and attachment to outline what he calls his ‘ TA theory of addiction’.
He contends that there has been an inadequate development of the Parent and Adult ego states resulting in a marked difficulty to self-soothe, set boundaries and limit the hedonism of the Free Child. He argues that ‘as a consequence the drug user will seek out another person or thing to take on the personality functions of her own Parent and Adult ego state and form a symbiosis with that. Drugs can do this well for some’ (p.57). He observes that listening to the dependent substance user talk about their relationship to their drug of choice is like listening to someone talk about ‘their husband or wife’. He also suggests that the symbiotic relationship may be with people, organisations or beliefs, citing an example of recidivist offenders who appear to only function well in prison. White then focuses on attachment theory, using research evidence to underpin his contention that certain kinds of problematic attachment are closely correlated to drug and alcohol dependencies in later life. He suggests that difficulties with separation/individuation and the formation of identity lead to the equivalent of a dependent personality disorder, where addicted drug users experience strong proximity-seeking behaviour and deep fears of being without their drug of choice.
Chapter Four offers a clear framework for assessing different types of substance use and misuse, from the experimental and recreational user at one end of the spectrum to the symptomatic and ‘true’ addict at the other. The author presents an overview of mainstream drug counselling responses for the first four types of drug and alcohol use, including some gems of clinical experience around working effectively with the Rebellious Child. Using the concept of the four ‘Ls’ – Liver, Lover, Livelihood and Legality, he offers a simple yet effective way for both the counsellor and the drug user to think about harm. For the last two types of use, the symptomatic and the dependent user, he argues that while both are addicted, their relationship to their drug of choice is different. He contends that symptomatic users are self-medicating, that their drug use is to solve a problem rather than being used in a habitual way, and that once the underlying difficulty eg PTSD, depression etc is attended to, their need for drugs dissipates.
Part Two outlines specific drug and alcohol techniques and interventions such as Harm Reduction Counselling, making a thorough Assessment, working with Ambivalence using Motivational Interviewing and how to work effectively with Relapse. The author’s work focuses on Relapse Process work rather than Relapse Prevention, as he suggests relapse is often inevitable and that coming off drugs is like leaving a relationship: it’s a process, often a painful one, with the varying degrees of difficulty reflecting the duration, intensity, quality and meaning that each relationship has. In this chapter, White writes compellingly of the ‘beginning of the end’ when the dependent drug user gathers enough momentum for change, where the drug counsellor is looking to heighten separation anxieties to enable their ‘psychological extraction’ from drug careers. He uses a number of touching case study examples to show the turmoil and emotional charge involved in letting go of this once crucial part of the client’s identity and existence.
The strengths of this book are in the author’s generous sharing of his clinical experience and wisdom and in his promotion of Transactional Analysis as an important resource to those working in drug and alcohol treatment services.
I had hoped to find relevant pieces of literature from the TA canon such as Jody Boliston-Mardula’s work on Appetite Paths (Boliston-Mardula, 2001), Robin Hobbes’ articles on TA and Attachment (Hobbes, 1997) and Jo Stuthridge on TA and Trauma (Stuthridge, 2006). Their lack of inclusion left me with a sense of theoretical incompleteness and insularity.
Trauma and PTSD are mentioned clinically but are surprisingly absent from theory. This matters, as White later hypothesises a difference between symptomatic drug use and dependent drug use, between people with addiction problems who have experienced trauma or have an underlying mental health problem and those who haven’t, a distinction in my experience that often doesn’t hold up. Stuthridge writes that trauma impairs the developing Adult ego state’s capacity for selfnarrative, resulting in disassociated ego states (Stuthridge 2006). These un-integrated aspects of self are then enacted with others again and again as the ‘traumatic script’ plays out. Rather than a lack of introjected adequate Parent and Adult ego states as Tony White suggests, an alternative perspective would suggest that there is a reliving of the original unsatisfying, abandoning or abusive relationship, a view that would certainly fit with the daily repeated experience of chaos and distress that is the dependent drug and alcohol user’s life
While researching my response to this book I became curious about the TA canon on drug and alcohol addiction, a story that was once central and now appears to have been marginalised. Indeed it was difficult to find the articles by Mardula and Hobbes as they are not included in our core publication, the TAJ. Given that addiction has been described as one of the most pressing public health emergencies facing westernised societies (Buchmnan et al., 2010), I am curious about why this discourse has fallen from favour, and grateful to Tony White for bringing this important and timely conversation back to the table.
References
Boliston-Mardula, J. (2001). Appetite Path Model. TA UK,
61 pp9-14.
Boyce, W.T. (2006). Symphonic causation and the origins
of childhood psychopathology. In Chichetti, D. & Cohen,
D.J. (Eds.), Developmental Psychopathology (2nd ed.) Vol.
2: Developmental Neuroscience (pp797-817). New York,
NY: John Wiley and Sons.
Buchman, D.Z. et al. (2010). The Paradox of Addiction
Neuroscience. Neuroethics 4(2), pp65-77. DOI
10.1007/s12152-010-9079-
Hobbes, R. (1997). Attachment Theory and Transactional
Analysis, Parts One and Two. (Retrieved from
http://www.elantraining.org/downloads.html#sh3).
(Originally published in ITA News, 46 & 47).
Shaffer, Howard J. (1986). Conceptual crises and the
addictions. Journal of Substance Abuse Treatment, 3,
pp285-296.
Stuthridge, J. (2006). Inside Out: A Transactional Analysis
Model of Trauma. Transactional Analysis Journal, 36(4),
pp268-283.
Jo Moores CTA, has a private psychotherapy practice in South Manchester. She has an interest in working with trauma using a combination of Transactional Analysis and EMDR, and enjoys working with couples. She worked at The Big Issue In the North for nearly a decade, working to improve services for homeless people and those struggling with drug and alcohol dependencies. Her web address is
www.psychotherapymanchester.com
Thursday, July 25, 2013
Suicide pact
In the city where I live, at the moment there is considerable media interest in an elderly couple who died. Apparently the man shot his wife dead, called the police and then shot himself dead before the police arrived. The police are trying to work out if it was a murder - suicide or a suicide pact. This raises some interesting points about suicide pacts that I discuss in my book - Working with suicidal individuals - where I note there are three types of suicide pacts shown in the diagrams below.

If the elderly couple had a suicide pact then it is the first type of suicide pact shown. Both parties want to die and agree to do so together. However certain things about this type of suicide should be publicly known. Both parties need to be equally involved in the preparations and act of making the suicide attempt. If the elderly man shot his wife dead, then shot himself but did not die then it is highly likely he would be charged with murder even if it was a suicide pact, (that is the wife wanted to die and wanted him to shoot her).
In the other two types of suicide pacts there is only one person who wants to die but the external party relates to the suicidal person in such a way that elevates the chance of a serious suicide attempt. The relationship between the two becomes supportive of suicide as a solution to the suicidal person’s problems and hence we have some kind of a pact.
As the second diagram shows some people take the view that suicide is a choice that a person has the right to make. It is everyones right to decide how and when to die. This is not an uncommon view held in the community, by a significant number of people and has logical and philosophical merit. If a suicidal person has a close relationship with the other who has these views then in one sense one could see this as a suicide pact. Not only is the suicidality being logically supported by the other but the suicidal person will also introject those views into their own Parent ego state, thus increasing the likelihood of a serious suicide attempt.
The third relationship occurs when the suicidal person has been suicidal for some time, may have even made an attempt and remains suicidal. Again not an uncommon scenario as for many, suicidality slowly increases over time, 75% tell others about their suicidal thoughts and the ratio of attempts to completed suicides varies from 1 to 40, up to 1 to 200.
Living with or having a close relationship with such a suicidal person is a very difficult and stressful thing to do. The non suicidal person can suffer greatly in this way, sometimes for years. Of course this person does not want to live like that and one way it is going to stop instantly and for ever, is if the suicidal person dies. If that happens then all that stress disappears instantly and forever (and the suicidal person knows this as well). It seems reasonable to conclude that any close person at some level wants the suicidal person to die as the Free Child in all of us would want the great stress to go away. Hence in this way the other supports the suicide of the suicidal person and hence we have the third type of suicide pact.

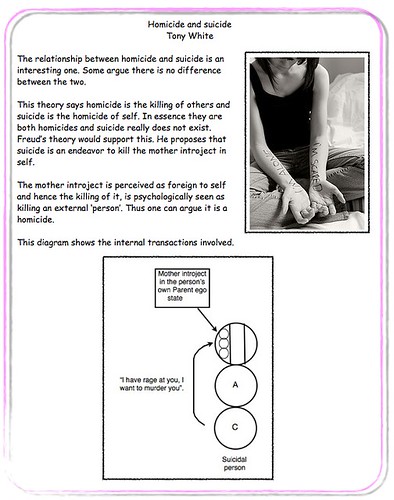
I discuss such case studies of this type in my book and this is where it gets murky and unclear. If one lives with a suicidal person, that is very stressful as I mentioned before. If that goes on for months or years does the non suicidal other begin to alter their behaviour consciously or unconsciously such that the likelihood of a completed suicide increases? Starting to not notice higher risk indicators, brushing off suicidal comments as just another one like the 30 before, altering behaviour such that the likelihood of finding the loved one making an attempt decreases. As I said before all of us have a Free Child and that ego state wants the horrible stress to stop, no matter how much we love the suicidal person. It could be argued that because of this everyone at some unconscious (or conscious) level would begin to act in such ways as just described.
Graffiti
Wednesday, July 24, 2013
Injunction - Don’t be you (the sex you are):
In this life script message the parents some how communicate to the child that they should have been born the opposite sex. A female may be born fourth in a line of girls as the parents tried to have a boy and this can leave the child with a deep sense of disappointment about itself. Some parents openly tell the child that she was meant to be a boy. They may dress the child as the opposite sex and engage it in activities of the opposite sex. The child maybe given a name that is usually used for the opposite sex or could be applied to the opposite sex. The child may be named after a relative who was the opposite sex. All these type of things can communicate to the child that it was meant to be born the opposite sex.
However it does not only have to relate to one’s gender. Some parents want their children to go to university and some simply do not have the academic ability to do so. Or the parents may want the child to be musical or sporty and the child has little talent and or interest in doing such a thing. Some parents put children in beauty or talent contests. Are they doing so for the child or because they want the child to be some way for their own psychological needs? In these instances the child again realizes that mother or father want them to be a particular way and realize they cannot or don’t have any interest in it and this can lead to emotional problems as described below.

We are who we are
It is possible for this injunction to lead to quite significant levels of maladjustment especially in the case of “Don’t be the sex you are” message. One’s gender is a basic and integral part of how people perceive and view them self. It is part of the core understanding of who we are. If they receive the message they should have been the other gender that can lead to quite a deep and profound sense of disappointment in relation to the parents and the child being in some cases disappointed in itself for some how not getting it right.
This injunction can be a basis of ego dystonic homosexuality and ego dystonic heterosexuality, some transvestism and some transgenderists. The DSM-5 would refer to this as a dissociative disorder where there is a disturbance in ones identity, in this case sexual identity. They note that such things can result from prolonged and intense coercive persuasion. One could see this as a euphemism for parenting in childhood which is a prolonged and intense period of persuasion.
This can also lead to pathological reasons for seeking cosmetic surgery. Repetitive cosmetic surgery can result from this injunction. Also there may be extreme fitness training as the person is trying to transform them self physically into something else, alternatively some have eating disorders for the same reasons.
They can also adopt the opposite gender role in relationships. Females will have more masculine qualities and less feminine qualities and the male is the other way around. So the male will adopt the traditional female roles in relationships and the female will adopt the male roles.
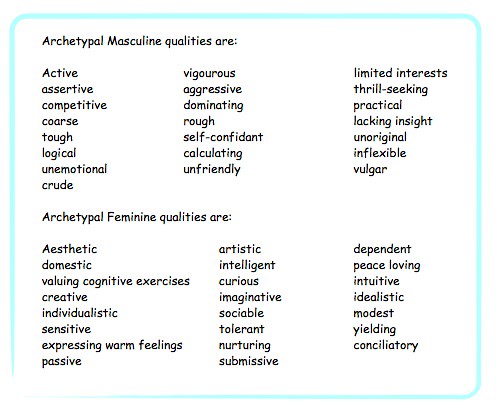
The tom-boy can be from a Don’t be you injunction. The parents wanted a boy and they got a girl so they treat her like a boy anyway. The girl adopts the typical male type of dress, activities, hobbies and employment. The same of course applies for the other way around when boys are treated like girls because the parents wanted a girl.
Others refuse to accept the age they are. They do not like getting older so they will adopt activities that are appropriate for younger ages, or they may ‘hang out’ with others who are much older or younger than them self. Some refuse to accept the aging in the body and will behave in a way that can at times be dangerous. For instance some men in their 60s will do heavy physical work or strenuous sporting activities that they could handle in their earlier 20s because they do not want to admit they are getting older and they still see themselves as a young person.
This can also give rise to what is called a chronophillia. That person who is sexually and romantically attracted to a person who is considerably older or younger. They just never fall in love with someone who is approximately the same age. This can be due to the fact that the parents let them know there was something wrong with who they were as a person, so they cope with it by changing their psychological view of self to fit with what the parents did want.
Graffiti
Tuesday, July 23, 2013
Subscribe to:
Posts (Atom)