(Originally presented in
“Thoughts on Shame”. The Transactional Analyst. The quarterly magazine of the Institute of Transactional Analysis. Summer 2012, Vol 2 (3), Page 21 - 24.)
Introduction
I have always found shame somewhat of a perplexing emotion. It has some unique features that separates it from the rest of the emotions especially in how one deals with it therapeutically. This has lead me to research and study this emotion and hence the motivation behind this article. Writing on shame abounds in the literature including Wright, Gudjonsson and Young (2008), Gao, Wang and Qian (2010) and Wolf, Cohen and Insko (2010). In the transactional analysis literature an excellent statement on shame is made in a theme edition on shame in the Transactional Analysis Journal (April (1994)). Including articles by the likes of Erskine (1994) and English (1994).
Shame the emotion
In surveying the literature on shame one quickly comes across a debate about the nature of shame and what it actually involves. In this article the terms emotion, feelings and affect are used interchangeably. One commonly finds three concepts mentioned in relation to shame - internalized anger, guilt and shame itself. There are differing views on these such that one finds confusion in the literature about the nature of and definition of shame. For example Goss and Allan (2009) in their discussion of shame state, "It blends the different emotions of anger, anxiety and disgust, involves social comparison and can have different foci,…"(p303-304). Others have disagreed with this and attempted to distinguish the various emotions involved with shame including guilt and anger, (See: Gao, Wang and Qian (2010) and Wright, Gudjonsson and Young (2008)). This is also well summarised by Wolf, Cohen and Insko (2010) who state, "What are shame and guilt, and how do they differ? Within psychology, as well as everyday conversation, the terms shame and guilt are often used interchangeably. There is a general confusion about the distinctiveness of these emotions, possibly because of their many similarities."(p337-338)
As mentioned before anger and guilt are often mentioned as relating to shame or being part of shame. My own view is that each of these constitute three separate psychological processes. They are three separate entities. However they can and often do occur contemporaneously. This could then explain why some see guilt as being part of the shame experience or internal anger being defined as shame on other occasions. If one can define the three separate psychological processes this would clarify the nature of shame and its associated processes. Fortunately Transactional Analysis theory allows us to come up with quite clear statements about the distinct psychological processes involved in each of these three emotions.
Internalized anger
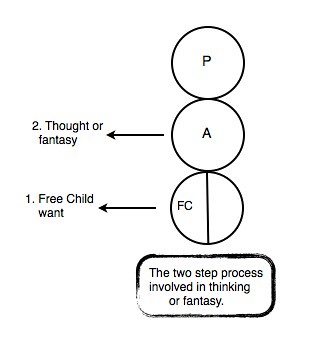
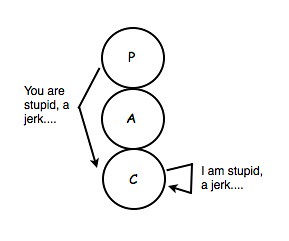
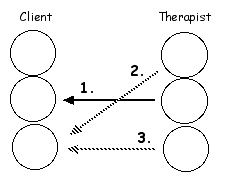
There are two ways in which internal anger can occur in ego state theory. See diagram 1.
Diagram 1
People can express anger at themselves from their Child ego state. When this occurs people will do negative internal self talk such as I am stupid, I was a geek talking to that girl and so on....
Anger can also be expressed from the Critical Parent ego state to the Child of the person. In this case the internal self talk starts with a “You” statement when an internal chastisement occurs. Examples may be “You were such a jerk talking to that boy”, “You can’t even get a simple report right”, “You stupid jerk” and so forth.
Guilt
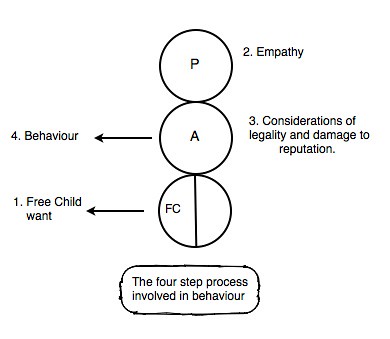
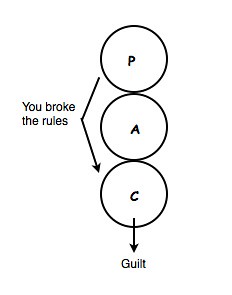
Guilt occurs when the person has a sense of breaking an internal rule which they have for themself. If a husband thinks the woman next door is hot and foxy but has a rule inside his Parent ego state which says, “Thou shalt not covet thy neighbour’s wife” then he can end up feeling guilt for having such thoughts.
Or a person may steal money from his brother and later feel guilt about it because he has the rule in his Parent that you don’t steal from your brother. People can feel guilty the next day after a night of drinking too much. Alcohol decommissions the Parent ego state and thus people behave in ways that they usually wouldn’t. The next day after the alcohol has worn off they feel guilty because the Parent ego state becomes active again. Diagram 2 shows the transactions.
Diagram 2
Shame
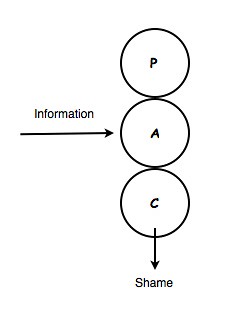
Finally we have shame which is a natural feeling reaction to particular environmental stimuli. Often, but by no means always, it is associated with sex, nudity or intimate bodily processes such as urinating or defecating. A prime example is the enuretic child who wets his bed at night. When the child wakes up and realizes he has wet the bed it is very easy for him to feel shame and he can go to extensive lengths to try and hide it. Indeed parents need to be very careful not engender a sense of shame in a child when he wets the bed. It needs to be dealt with carefully so as to avoid this. What is being suggested here is that shame is one of the innate feelings that all humans can experience. Others such as Adams (2008) and Kaufman (1992) have suggested the same. In this way shame is a natural Free Child reaction to certain events. Thus we have the shame transaction in diagram 3.
Diagram 3
As you can see this differs from the guilt transaction in that there is no Parent to Child transaction before for emotion is experienced. This is consistent with Freud’s presentation on shame which is probably best summed up by Lynd (1958) who notes that guilt is usually more related to transgressions of clear moral codes and rules. No better example of this is found in religious texts which define what behaviors, thoughts and feelings are regarded as sinful. These are incorporated into the Parent ego state by the young child and when transgressed the individual most often will experience guilt.
With shame the rules are much less codified and clear. Transgressions of them are more by tactlessness, errors in taste or bad luck. As a result the Parent ego state is much less involved in the process. Again the example of the enuretic child demonstrates this. Wetting the bed does not break a Parent ego state rule and generally would not be regarded as sinful. Instead it results from bad luck or factors outside the child’s control.
Presented here are three separate psychological processes – inward directed anger, guilt and shame. They can occur on their own or they can occur together. However if we see them as separate processes then we are afforded the opportunity to understand shame without the usual confusion of guilt and inward directed anger.
Unique qualities of shame
What does a therapist do when a client presents with feelings of shame? One knows what to do when a client is angry. They feel the anger, they express the anger and when ready they drop the anger. When a client feels sad the therapist acknowledges the feeling, the client expresses the sadness with some kind of crying usually, one listens to the client, empathizes with them and is compassionate. Then the sadness is dealt with.
The natural Free Child reaction to anger and sadness is a therapeutic one. There is a natural desire to talk about it, to have some kind of catharsis and release the emotion. This natural urge will result in the feeling being ‘worked through’ often with the support of a compassionate other. The feeling is naturally dealt with and resolved which of course is a desirable state of affairs and makes the therapy process clear.
However shame is different. When people feel shame there is a strong desire to withdraw or change the topic. The person wants to go into hiding in some way. Common bodily expressions when one experiences shame include a bowing of the head, an attempt to hide the face possibly with the hands, a blushing of the face, possible sweating, body bent over on itself and possibly a closing of the eyes. It’s like the person is endeavoring to make them self as small and invisible as possible and there is a strong drive to isolate self. This seems to be the natural Free Child reaction to shame. The problem with this, is it does not deal with it in the therapeutic sense unlike anger and sadness.
In essence it is an avoidant, ‘Lets try and forget about it’, approach. Therapeutically this does not resolve the difficult feelings. They need to be brought out into the open, experienced and then one can ‘get over it’. The Free Child reaction with shame is to hide and avoid. With most other feelings the Free Child reaction is a therapeutic one that will bring resolution of the painful event like expressing sad feelings when one’s cat dies. With shame the natural Free Child reaction will not bring resolution or closure to the event. Thus shame is somewhat unique in this way.
Society likes a temperate woman
Working with shame in the therapeutic process.
Paradoxically therapists are often working with shame even before being aware they are. For instance clients with bulimia or those who self harm often feel shame about their behaviour. As the natural response to shame is to hide often the client will not disclose such behaviour for some time. The goal here is to establish relational contact such that the client feels ready to disclose what they see as shameful behaviour but the therapist will only know that in retrospect. However when the client does finally disclose such feelings then one knows that successful relational contact with the client has been established. White (1998) discusses this in detail in his paper on transference and humanness of the psychotherapist. Such transferential and counter transferential contact is made when the therapist allows himself Free Child ego state contact with the client. This as he points out is surprisingly difficult to do but if done then the transference established will promote the client to expose their sense of shame to the therapist. Thus achieving one of the first crucial steps in working with shame in the therapeutic process.
The next step in this method of working with shame is to diagnose what is actually happening. As I said before shame, guilt and inward anger are often confused. The therapist needs to question the client to ascertain which of the three processes is occurring to see if the person is actually experiencing shame. Indeed one of the indicators that shame is present is the fact that the person has been reluctant to bring it up. Often there will be more than one process occurring concomitantly. Once established this can be explained to the client so they are aware of what is actually happening with their emotions in this way. Which of the three processes they are actually experiencing.
If inward anger is diagnosed then of course the therapist deals with that appropriately as he does if guilt is indicated. The main problem emotion here is shame because as I mentioned before the natural Free Child reaction to shame is not a therapeutic one.
The therapeutic response I have developed is really quite simple. As the natural response to shame is to go into hiding one invites the client to do the opposite. To come out of hiding and bring the behavior and feelings of shame into the relationship with the therapist. Basically they talk about it and the therapist responds in an empathetic way, also disclosing their Child reactions to the behaviour and feelings of shame. The therapist expresses his Free Child responses to what the client is saying. The goal is to normalize the shame response in the client.
Once the client has made such a disclosure the therapist can also raise the events at the appropriate times. One needs to be somewhat forthright in this way as this assists the normalizing process. The more it is brought up, talked about in an open way with no ‘shock and horror’ responses from the therapist the less shameful it becomes. The shame loses its potency over time. If the therapist always waits for the client to bring it up then the normalizing process can be very protracted. If mentioned only very occasionally there may be little if any normalizing occurring at all.
Often the therapist needs to be proactive here and raise the shame producing events especially if the client never initiates talking about it. This is where clinical skill comes to the fore. One does not want to be always bringing it up but it does need to be raised from time to time. How often that is, depends on the client and the circumstances. If successfully managed then over time the shameful event becomes something that can be easily discussed with little or no shame reaction. At this point it can be said that the shame has been worked through.
Conclusion
While the Free Child of the client has a natural drive to work through feelings like anger and sadness this is not the case with shame. Hence the therapist needs to intervene to halt the natural hiding away reaction by the client to their shame. The therapist brings out the shaming experiences at appropriate intervals, they are discussed and over time the potency of the shame significantly reduces such that open discussion can occur and there is little sense of shame in the client.
References
Adams, S.A. (2008) “Using transactional analysis and mental imagery to help shame-based identity adults make peace with their past.” ADULTSPAN Journal. 7, 1, 2-12
English, F. (1994) "Shame and social control revisited." Transactional Analysis Journal. 24, 2, 109-120.
Erskine, R.G. (1994) "Shame and self righteousness: Transactional analysis perspectives and clinical interventions." Transactional Analysis Journal. 24, 2, 86-102.
Gao, J. Wang A. and Qian, M. (2010) "Differentiating shame and guilt from a relational perspective: A cross cultural study." Social Behaviour and Personality. 38, 10, 1401-1408.
Goss, K. and Allan, S. (2009) "Shame, pride and eating disorders." Clinical Psychology and Psychotherapy. 16, 303-316.
Kaufman, G. (1992) Shame: The Power of Caring (3rd ed.). Rochester, VT: Schenkman Books.
Lynd, H.M. (1958) On Shame and the Search for Identity. London: Routledge & Kegan Paul.
Wolf, S.T., Cohen, T.R. and Insko, C.A. (2010) "Shame proneness and guilt proneness: Toward the further understanding of reactions to public and private transgressions." Self and Identity. 9, 337-362.
White, T. (1998) "Psychotherapy and the art of being human." Transactional Analysis Journal. 28, 4, 321-330.
Wright, K., Gudjonsson, G.H. and Young, S. (2008) "An investigation of the relationship between anger and offence-related shame and guilt." Psychology, Crime & Law. 14, 5, 415-423.