I was reading a research report on police and stress as I have a bit of time to read such things over the festive season. It was saying that many who enter the police force self select in that they are looking for a stressful job as indeed being a police officer is. That reminded me of a question I was asked some time ago.
I was asked, “What was it like working in a prison?”
My answer, “I liked it because it was exciting. There is always the threat of physical violence in the air”.

This just kind of came out of my mouth and I didn’t even realise I thought it until I said it. Probably not the most politically correct answer in the world but it does indicate that I was self selecting for a stressful job.
And it is true there was always the threat of physical violence and whenever I was in the presence of inmates there was always a kind of hypervigilance on my behalf and I kind of liked that. Especially for me because the inmates that I usually dealt with were experiencing some kind of distress or psychological pain.
The most common form of physical violence that happened was usually inmate on inmate. Two prisoners had a physical fight for some reason. However inmate on staff member violence also happened at least every week or so but it was less common.
Even just entering the prison set the stage. You walk up to this large complex of buildings to enter through the gatehouse. On either side are wire fences, electrified fences and these long circular tubes of endless razor wire all over stretching for hundreds of meters. It actually presented quite an engaging scene. The fenced area is immaculately kept. All the lawns are mowed, there is no rubbish or objects lying about and all the wire and razor wire have that clear shiny stainless steel look to it. There was never any rusted wire.
I always thought you could get some great photographs with perspectives looking along the fence and long tubes of razor wire. But of course permission would never be granted to take such photographs.
Only once did I feel there was some kind of physical threat made directly to me but I backed off, talked my way out of it and it defused into nothing. There were verbal threats made on staff but these were also not so common as they would likely result in the prisoner being charged. I recall one prisoner threatened to have his friends on the outside kill the family of a staff member who I knew quite well.
Those inmates who wanted to threaten would most often do so more subtly. If he was a big man he may stand close to you and kind of lean over a bit. Others who had done particularly unpleasant crimes may recount them in loud detail to you seemingly relishing in what they had done. Most often this was just to test you to see how ‘hard’ you were. If you took it with disdain then they would respect you and that was the end of that.

I always never compromised my physical safety. Because of my role I had access to all the inmate files and whenever meeting an inmate unknown to me I would have a detail read of their crimes and how they handled prison life. Had they been on any charges in the past and so forth.
If I felt there was some risk then I would have an officer with me in the interview room when we met. There was few times when there were two officers in the room with me and the inmate. I always found this some what farcical. How can you counsel someone with one or two large prison officers standing behind him. With a couple of very violent men they were standing right at the side of us, almost inbetween!
One thing that did surprise me was that never did any prisoner ever question this. Not once did anyone ever say, “What are they here for?”, or “They don’t need to be here”. How can you counsel an inmate when there is no confidentiality and by me requesting the officer be there shows I have little trust of the inmate not attacking me. How does that impact on the therapeutic alliance. Well you can hardly call it an alliance, can you?
But my answer was true. I did find it exciting and that did appeal to me and made the work more fascinating and interesting to me.
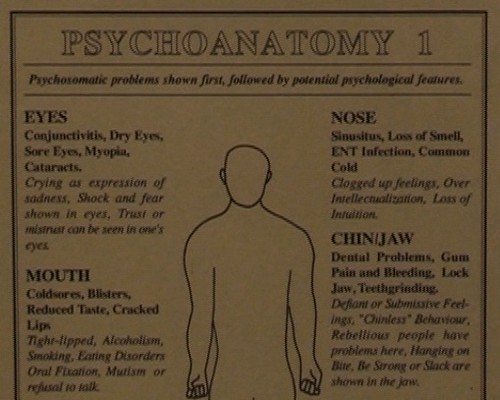
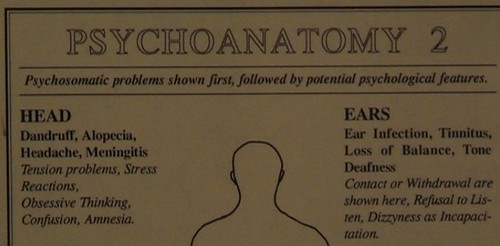
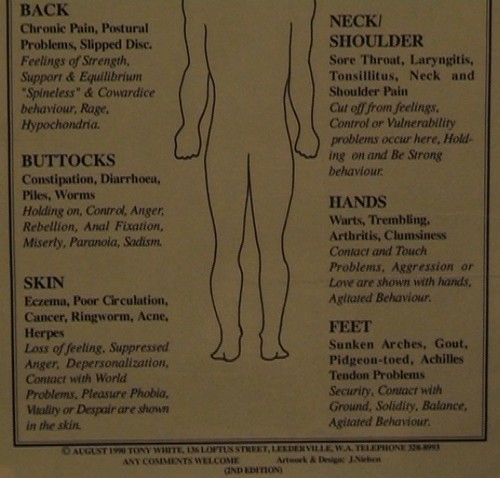
Graffiti