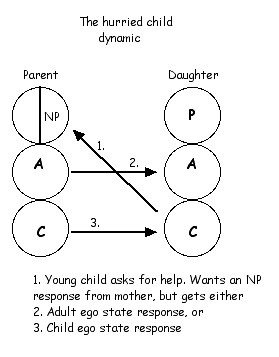
A child falls over, cuts its knee and seeks out mother for assistance. The youngster asks for help in the first transaction. The child has two problems, first it has the physical problem of a cut knee that needs a bandage put on it. Second it has a psychological problem. It is experiencing pain, perhaps shock of the fall and then the sight of the blood and it is generally feeling distress.
To respond successfully to the request the parent must at some point respond from their Nurturing Parent ego state to solve the psychological problem and the Adult to solve the physical problem. The hurried child syndrome occurs mainly when the psychological problem is not dealt with. Some parents do not do this and this can occur in a variety of ways.
1. The parent simply not respond at all. The mother may be in bed suffering severe PND and is simply too depressed to respond. The mother may be alcohol or drug affected which also does not permit her to respond or there may be some kind of severe mental illness or she is simply so consumed with her own emotional torment that she cannot respond.

Body language of a competent parent?
2. Others may respond but only from the Adult ego state. The physical wound is tended in the proper way, but it is done is a purely problem solving way with no nurturing involved. The psychological problem is left unsolved.
This most often occurs in parents who do parenting by the book. They will have a manual or some kind of book on parenting. When a difficulty occurs they will seek out the manual to find out what the author says is the right way to respond to it. It typically has chapters on discipline, toiletting, use of a dummy or not, getting a child to sleep, eat and so forth. Good information to have indeed but it is only Adult ego state and may reflect an insecurity in the person about their parenting.
3. The parent responds from their own Child ego state. In this case the youngster will feel unsatisfied because the parental response is child like and has no competent grownup nurturing quality to it. The parent responds from their own Child ego state with some kind of magical thinking about how to treat a wound or may simply try and jolly the youngster in some child like way.

Some parents are dominated by their own Child ego state
If there is no competent Nurturing Parent and Adult ego state response then the child is forced to hurry up and grow up emotionally. The most common reaction to this is one of anxiety. The child has a sense of being emotionally alone in the world and there is no big person around that they can emotionally rely on. There may also be some anger but the primary response is one of anxiety and scare.
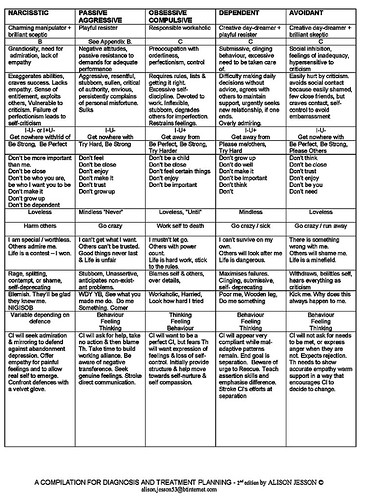
Below is a list of personality types. The hurried child dynamic can occur in most of them but is more likely in a some than others. Obviously it will be more common in those that tend to be anxiety based personality types. This will include:
Obsessive/compulsive
Schizoid
Schizotypal
Avoidant
Personality type Adaptation
Paranoid The world is hostile so don’t trust anyone and deal with people by being angry and attacking
Schizoid The world is scary so withdraw from it (people) and don’t show any of your feelings
Schizotypal The world is scary so withdraw from it (people) and don’t think clearly by being a bit crazy
Antisocial You can’t trust anyone & life’s unfair so take advantage of people and do what you like
Borderline Relationships & life are very unreliable so frantically do anything to keep people around
Histrionic I must be the centre of attention so I will be dramatic, flirtatious and highly emotional
Narcissistic I have always been told that I am very important and the best so I will behave and feel like that
Avoidant Life is scary and rejecting so I will withdraw and feel worthless
Dependent I can’t cope with life and am worthless so I will cling to others and do what they tell me
Obsessive/compulsive I have to feel in control of life and myself so I will be orderly and perfectionistic
Graffiti