Most commonly there is a single episode
Mortality rates are around 10%. One needs to be careful of this figure as it relates to people who are formally diagnosed as anorexic. There are many who have anorexic features who would not meet the formal definition. If you include these as well then it will be much less than 10%.
95% of anorexics are female
Common psychological factors
Results from oral stage of development problems. It results from the earliest development stage 0 - 18 months. Counselling needs to deal with oral stage issues.
Possibility of sexual issues. The woman is turning her self into a non sexual being. Whilst they may say that thin looks attractive the Child ego state aspect of her personality knows that being very thin is not attractive at all and thus no man will approach her sexually. (Some obese women can do the same with weight). They are also making themselves almost physically unable to get pregnant and to carry a child. Counselling needs to deal with the “Don’t be sexual” injunction and their thoughts and feelings of self as a sexual being. This will need to include an assessment of any parental messages about sex and the child becoming a sexual being. Anorexia in essence desexualizes the the girl or young woman making her a non sexual being by infantilizing herself. Also probably a “Don’t get your needs met” injunction.

Pro-ana
Family emeshment. Family subsystem boundaries are weak and easily crossed, members intrude on others. There may be over protectiveness where a symbiosis does not allow the child to develop competence to deal with the outside world. Cognitive and behavioural infantilization by parents. Counselling needs to address Adult and Parent ego state development and the establishment of boundaries.
Suicidal behaviour. Death from anorexia can be viewed as a suicide. One needs to make an assessment of the anorexic and the suicide decision (Don’t exist injunction). Then work with the self destructive part of the individual.
(TAJ 1985 was a theme edition of eating disorders. Whilst it is old it does have some good material in it) Lois Achimovich writes on anorexia, parental depression and the suicide decision. She notes that often the mother or father report chronic depression and suicidality. One also needs to make an assessment of depression in the anorexic.
Pre morbid personality - obsessional, perfectionism and need to conform covering a highly rebellious individual. Possibility of a personality disorder and a third degree impasse
In counselling one needs to avoid the RC of the client. A RC can only exist if the other party (therapist ) is CP.
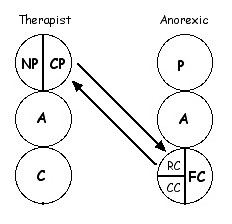
One needs to avoid this at all costs and this can be very hard to do at times as the client will try all sorts ways to entice the therapist into this set of transactions. If the therapist can avoid it then the anorexic relationship can not be established.
As anorexia has its origins from the oral stage of development they will be receptive to transference based approach to counselling. Often they will quickly see the therapist as a parent type figure and thus the transference neurosis will play out. As the client forms an attachment to the therapist they will be very sensitive to emeshment type of relating and expect the therapist to relate to then in an infantilizing way.
One will get contradictory transactions form the client. Some of the transactions from the anorexic will invite the therapist to emesh and infantalize them. If the therapist obliges initially this may be well received but eventually the client’s RC will kick in and then the anorexic relationship will be played out again.

Dinner time
If the therapist does not oblige and ‘rejects’ such invitations by the client they may initially get a hostile reception but if maintained in the longer term the client will experience the benefits from it.
One would also be suggesting ways by with the anorexic can stimulate themselves orally. Thus using a pacifier or thumb sucking in bed at night or even as the therapist does holding work with them. It may take some time before the client will agree to such a thing.
This may sound like the therapist is infantilizing the client. The therapist does invite the client to at times be quite regressed such as with holding work or making homework contracts to suck their thumb and so forth. However such regressions are for a specific therapeutic goal as I have described. Overall however the therapist expects (one could even say demand) that the anorexic solve her own day to day problems, resolve their own conflicts and so forth.
To further address the oral stage fixation one could also get the anorexic to place something in their mouth like a small marble which they can play with in their mouth for extended periods of time. Others usually do this with something like chewing gum but the anorexic wont agree to that because it would result in calorie intake. A small marble obviously will not result in any calorie intake and this can provide the person with ongoing oral stimulation. In addition it gets the anorexic used to the feel of having something in their mouth.
Graffiti
I was trying to remember a particular psychological term today after a client. And, after reading your blog just now, it came to me Tony. "Hostile Dependancy" is the phrase and a very good one at that.
ReplyDeletek
Yes kenoath,
ReplyDeleteI concur it is a good term indeed.
Nothing like a bit of hostility
Graffiti
There isn't much written about middle age onset eating disorders, but I have read that it isn't as uncommon as one might think. Aging sucks in so many ways for people who are already suffering from mental illness or even just low self esteem. It seems like we have no control over what happens to our bodies in middle age. I don't meet the criteria for an eating disorder, but I can tell you that I am at the stage where food is an enemy to me. But I certainly don't relate to the typical population of eating disordered women.
ReplyDeleteHi Harriet,
ReplyDeleteBeing middle aged myself I understand what you are saying about loss of control about what happens to our bodies. I see some men of my age try to take control and become obsessed with exercise and body. Not a good way to go I think and it just highlights what you say about the fear assocaited with the loss of control
Tony
anyone know of any studies about weight gain/loss after parents die?
ReplyDelete