Email received 27.7.11
Dear Tony,
I am delighted to inform you that your book Working with Suicidal Individuals has been highly commended in the Psychiatry category of the 2011 BMA Medical Book Awards. This means that you are shortlisted to win first prize in this category, and are invited to the awards ceremony.
Congratulations!
The ceremony will take place on Wednesday 14th September at BMA House in London, starting at 5.30pm. Please let me know if you would like to attend, and I will register this with the event organizer, and send you more details. I appreciate that since you are in Australia, this may not prove possible, but our commissioning editor will be attending to collect your award if necessary.
With best wishes,
Jessica Kingsley Publishers - 24 years of independent publishing 1987-2011
116 Pentonville Road, London N1 9JB, UK
Tel: +44 (0) 20 7833 2307 Fax: +44 (0) 20 7837 2917
------------------------------------------
But guess what!
About a month ago I booked the flights to be in the UK from September 6th to 17th!
Is this divine intervention?
Or just plain divine?
I will have to make sure I cry at the right time and have a long list of thank you’s to say!
------------------------------------------
An article involving the psychological examination of three suicide notes - Adolf Hitler, Virginia Woolf and Sid Vicious of the Sex Pistols found here.
Order form for book can be found here.
------------------------------------------
The list of universities and colleges that now stock the book in their libraries for courses in psychology, counselling, social work and nursing continues to grow as well.
Maribor General Hospital Library (Slovenia)
Stellenbosch University Library (South Africa)
Mitt hogskolan library (Sweden)
Stockholm University (Sweden)
PJ Library (Norway)
University of Bergen (Norway)
Norges teknisk-naturvitenskapelige universitet (Norway)
University of Oslo (Norway)
University of Tromso (Norway)
University of the West of England (UK)
University of Plymouth (UK)
Manchester Metropolitian University (UK)
Lancaster University (UK)
University of Hull (UK)
University of East Anglia (UK)
University of Cambridge (UK)
Oxford University library (UK)
University of Exeter (UK)
Coventry City Council library (UK)
Bromley Library service (UK)
Cadbury Heath Library (UK)
Kingswood Library (UK)
Yate Library (UK)
British Library (UK)
Ebook library London (UK)
Hounslow Library (UK)
Barnet London Borough Library (UK)
National library of Scotland (Scotland)
Executive Counseling and Training Academy (Singapore)
Ngee Ann Polytechnic Library(Singapore)
Singapore Polytechnic Library (Singapore)
National University of Singapore (Singapore)
LaTrobe University (Aust)
Victoria University (Aust)
Queensland University of Technology (Aust)
Deakin University (Aust)
University of Western Australia (Aust)
University of Ballarat (Aust)
University of New England (Aust)
University of Western Sydney (Aust)
Charles Sturt University (Aust)
Curtin University (Aust)
Australian Catholic University (Aust)
University of Newcastle (Aust)
Bond University (Aust)
University of Melbourne (Aust)
James Cook University (Aust)
National Library of Australia (Aust)
University of California San Diego (USA)
Open Library. California State Library (USA)
Marquette University Raynor Memorial Library (USA)
University of Massachusetts Amherst (USA)
Williams College Massachusetts (USA)
National Library of Medicine Maryland (USA)
Illinois State University (USA)
Loyola Marymount University California (USA)
University of Michigan (USA)
Central Michigan University (USA)
University of North Carolina Chapel Hill (USA)
University of Missouri-Columbia (USA)
Akron-Summit County Public Library, Ohio (USA)
University of California Merced (USA)
University of North Carolina Greensboro (USA)
Library of congress (USA)
University of California San Franisco (USA)
Mt. Hood Community College Library Oregon (USA)
National College of Natural Medicine Oregon (USA)
Oregon Health and Science University (USA)
Northeast WI Public Libraries (USA)
College of DuPage Illinois (USA)
Boston College (USA)
University of Chicago Illinois (USA)
University of North Texas (USA)
Laredo Public Library Texas (USA)
University of Texas-Pan American (USA)
University of Texas at Austin (USA)
Trinity College Dublin (Ireland)
Dublin Institute of Technology (Ireland)
University of Auckland Library (New Zealand)
Auckland University of Technology (New Zealand)
Unitec Institute of Technology (New Zealand)
Eastern Institute of Technlogy (New Zealand)
University of Otago (New Zealand)
Rotorua District Library (New Zealand)
University of Waterloo (Canada)
Mount Royal University (Canada)
Wilfrid Laurier University (Canada)
University of Guelph (Canada)
Library and Archives Canada (Canada)
City University of Hong Kong (China)
National Cheng Kung University (Taiwan)
Graffiti
Thursday, July 28, 2011
Monday, July 25, 2011
The contextual diagnosis of ego states
Introduction
Eric Berne (1961) in his book Transactional Analysis in Psychotherapy outlines the four ways by which the diagnosis of ego states can occur
Behavioural diagnosis - This is the most common method used and involves the observation of a person behaviour, body language, voice, demeanours and so forth.
Social diagnosis - This involves observing the types of communications or transactions the person has with others. How others respond to him give some indication of the ego state in which he may be.
Historical diagnosis - This involves enquiring into the persons history. How they acted and responded in their past will give insight into how they are responding in the here and now.
Phenomenological diagnosis - This is the diagnosis of ego states by self examination. An awareness of ones feelings and current experience can be used to assist in the correct diagnosis of ego states.

The need for a contextual diagnosis
For many years psychologists have examined the role of context in human psychology. It is now a widely held belief that humans examined in the context in which they exist will give a much more comprehensive understanding of them.
Indeed context is integral to how we perceive the world, even down to the perception of simple basic objects. This is no better illustrated than with the Rubin vase. When presented with an ambiguous object (ie with no context) humans can fluctuate in what they are actually perceiving. See the Rubin vase below. Some people see a vase, others see two profiles and yet others fluctuate between the two.

Rubin vase
Add in some context and the perception of the figure becomes far more consistent. In the picture below some context has been added such as depth perception and other markings on the object. The vast majority of people will now see a vase rather than two profiles.
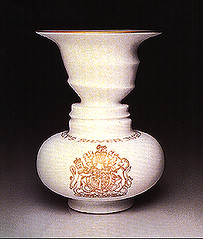
The Rubin vase illusion is important because it shows that perception is not solely determined by the image formed on the retina. Thus the very way we see the world is determined by the context of what we are looking at. This of course highlights the integral importance of context in how humans interact with the world.
At the macro end of the scale we have the discipline of social psychology. This whole approach to psychology is based on the assumption that to understand people one has to examine the context in which they live and operate. To view a person in their wider context allows one to gain a fuller comprehension of why they do what they do and indeed who they even are in the psychological sense.
The point at hand here is to demonstrate that from the micro to the marco of human functioning we see the importance and value of context. Thus it is proposed that to diagnose ego states accurately one needs to do a contextual diagnosis. Examples of how this diagnosis works are plentiful and easy to demonstrate.
Contextual diagnosis
A man says, “On July 5th, 2007 the alignment of the planets will create a magnetic field so large that there will be the biggest tides in half a century”. What ego state would be diagnosed?
If that man was of a dishevelled appearance, not shaven for 2 days and was
sitting on a park bench drinking out of a bottle in a brown paper bag what ego
state would be diagnosed?. Probably some kind of regressed Child ego state. If
that man was in an observatory wearing a white coat and carrying a clip board
what ego state would be diagnosed? Probably Adult ego state. The different
contexts for the same statement would tend to result in a different diagnosis.
The context in which the statement is made is central to the diagnosis of ego
states.
Thus one has the fifth way by which ego states can be diagnosed - The contextual diagnosis.
Ego state diagnosis on basis of body
language with very little context?
Possibly perplexed Adult ego state or maybe Adapted Child ego state in some slight discomfort or pain after playing a game.

Ego state diagnosis on basis of body language
within the context of his immediate milieu?
Eye strain with probable Free Child ego state sexual arousal.
References
Berne, E. 1961.
Transactional Analysis in Psychotherapy. Ballantine: New York
Graffiti
Eric Berne (1961) in his book Transactional Analysis in Psychotherapy outlines the four ways by which the diagnosis of ego states can occur
Behavioural diagnosis - This is the most common method used and involves the observation of a person behaviour, body language, voice, demeanours and so forth.
Social diagnosis - This involves observing the types of communications or transactions the person has with others. How others respond to him give some indication of the ego state in which he may be.
Historical diagnosis - This involves enquiring into the persons history. How they acted and responded in their past will give insight into how they are responding in the here and now.
Phenomenological diagnosis - This is the diagnosis of ego states by self examination. An awareness of ones feelings and current experience can be used to assist in the correct diagnosis of ego states.
The need for a contextual diagnosis
For many years psychologists have examined the role of context in human psychology. It is now a widely held belief that humans examined in the context in which they exist will give a much more comprehensive understanding of them.
Indeed context is integral to how we perceive the world, even down to the perception of simple basic objects. This is no better illustrated than with the Rubin vase. When presented with an ambiguous object (ie with no context) humans can fluctuate in what they are actually perceiving. See the Rubin vase below. Some people see a vase, others see two profiles and yet others fluctuate between the two.
Rubin vase
Add in some context and the perception of the figure becomes far more consistent. In the picture below some context has been added such as depth perception and other markings on the object. The vast majority of people will now see a vase rather than two profiles.
The Rubin vase illusion is important because it shows that perception is not solely determined by the image formed on the retina. Thus the very way we see the world is determined by the context of what we are looking at. This of course highlights the integral importance of context in how humans interact with the world.
At the macro end of the scale we have the discipline of social psychology. This whole approach to psychology is based on the assumption that to understand people one has to examine the context in which they live and operate. To view a person in their wider context allows one to gain a fuller comprehension of why they do what they do and indeed who they even are in the psychological sense.
The point at hand here is to demonstrate that from the micro to the marco of human functioning we see the importance and value of context. Thus it is proposed that to diagnose ego states accurately one needs to do a contextual diagnosis. Examples of how this diagnosis works are plentiful and easy to demonstrate.
Contextual diagnosis
A man says, “On July 5th, 2007 the alignment of the planets will create a magnetic field so large that there will be the biggest tides in half a century”. What ego state would be diagnosed?
If that man was of a dishevelled appearance, not shaven for 2 days and was
sitting on a park bench drinking out of a bottle in a brown paper bag what ego
state would be diagnosed?. Probably some kind of regressed Child ego state. If
that man was in an observatory wearing a white coat and carrying a clip board
what ego state would be diagnosed? Probably Adult ego state. The different
contexts for the same statement would tend to result in a different diagnosis.
The context in which the statement is made is central to the diagnosis of ego
states.
Thus one has the fifth way by which ego states can be diagnosed - The contextual diagnosis.
Ego state diagnosis on basis of body
language with very little context?
Possibly perplexed Adult ego state or maybe Adapted Child ego state in some slight discomfort or pain after playing a game.
Ego state diagnosis on basis of body language
within the context of his immediate milieu?
Eye strain with probable Free Child ego state sexual arousal.
References
Berne, E. 1961.
Transactional Analysis in Psychotherapy. Ballantine: New York
Graffiti
Sunday, July 24, 2011
Amy Winehouse
Rest In Peace Amy

A lot of people told you how they thought you should live your life but you did it your way. I wish you were still here and I admire you for living the life you did. And thanx for the really good music!
Graffiti
A lot of people told you how they thought you should live your life but you did it your way. I wish you were still here and I admire you for living the life you did. And thanx for the really good music!
Graffiti
Ego states in the counselling process
Three new articles have been uploaded. I would have done it here but Blogger cannot take Pdfs.
Number 1
The Child ego state in counselling
Paper 1 – Looking for the Child ego state in counselling
How Child is brought into the counselling session
1. Feelings
2. Contracts for taking the client out of their comfort zone.
3. Polarities.
Conclusion
Paper 2 – Psychological polarities
Paper 3 – Relational contact with the AC

Number 2
Parent ego state
The Parent ego state
Sameness in relationships
How modelling occurs
Group think

Number 3
Working with the Conforming Child, Rebellious Child and Free Child ego states
The highly conforming client
The highly rebellious client
Dealing with the difficult client – Free Child, Conforming Child & Rebellious Child
Pdf here.
Graffiti
Number 1
The Child ego state in counselling
Paper 1 – Looking for the Child ego state in counselling
How Child is brought into the counselling session
1. Feelings
2. Contracts for taking the client out of their comfort zone.
3. Polarities.
Conclusion
Paper 2 – Psychological polarities
Paper 3 – Relational contact with the AC
Number 2
Parent ego state
The Parent ego state
Sameness in relationships
How modelling occurs
Group think
Number 3
Working with the Conforming Child, Rebellious Child and Free Child ego states
The highly conforming client
The highly rebellious client
Dealing with the difficult client – Free Child, Conforming Child & Rebellious Child
Pdf here.
Graffiti
Friday, July 22, 2011
Newspaper articles about adolescence


Friday, July 15, 2011
Childhood mental health problems
Most common mental health issues encountered in 6 to 12 year olds
Reported by school psychologists
Anxiety - 73.1%
Challenging behaviour - 71.8%
Family/parenting concerns - 65.4%
Peer relationships - 59%
Anger and conflict - 55.8%
Bullying - 41.7%
Self esteem - 38.5%
Child safety and protection - 31%
Depression - 21.1%
Trauma - 19.2%
Challenging behaviour = Autism spectrum disorder, ADHD, oppositional disorder, learning difficulties and conduct disorder
Ref: [Inpsych - Bulletin of the Australian Psychological Society, June 2011]

My work with children has mainly been in the private practice setting. Children are brought to me by their parents usually. The list cited above would be quite similar to how I would rate the children I have seen over the years.
One thing that has always interested me in my work with children, and what this data supports, is the low rate of depression as compared to the other mental health problems presented. I have found this surprising as I expected it to be higher. I expected anxiety to be as high as it is but I also expected depression to be the same. Which it is not. The rate of depression is much lower.
Why I expected this is because with adults and adolescents they tend to be about the same.
Adults in Australia (Department of health and ageing statistics)
10% anxiety at some point in adult life
20% depression (6% major depression)
One needs to be careful with such statistics as they can vary quite considerably depending on how one defines depression and anxiety. However, it seems safe to say that in adults there are similar amounts of depression compared to anxiety unlike in childhood. They are at similar rates whereas in childhood that is not the case with anxiety being much more prevalent than depression. According to the research above anxiety is three to four times more prevalent than depression in children seeking help from school psychologists.

This of courses raises the question as to why this would be so. I don’t know of any explanation that has been given to answer this question. So I thought I might do some hypothesising of my own.
Anxiety in childhood
It could be that diagnosing depression in children is harder than in adults. Thus the rates of depression are higher in children but are not recognised because the children do not present to school psychologists with that difficulty. I suppose this could be the case but it seems a bit dodgy to me as depression is not that hard to diagnose. Even if the child does not report the problem emotions found in depression the body language of a depressed child is not that hard to detect. It would also seem reasonable that a depressed child is just as likely to report unpleasant emotions as an anxious child. Why should there be any difference between those two?
It seems more reasonable to me that childhood by its very nature is more likely to produce reactions of anxiety rather than depression, whereas in adulthood this is not the case. It is simply a matter of when god made us, she stuffed up. The way humans reproduce the species is by giving birth to very small versions of adults that take almost two decades to fully mature.
As adults it is easy to forget just how vulnerable a child is. A child is like living in the land of the giants. Take a minute to lie face up on the floor, get someone to stand over you and remind yourself of how a child sees her relationships with adults.
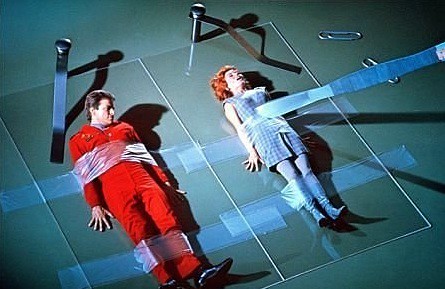
One of my favourite TV shows in childhood - Land of the giants.
This could partly explain why anxiety is the highest of all mental health issues in childhood. A child’s life is on the line each day. Its actual physical existence is out of its control and is determined by those adults around her. Indeed a threatening state of affairs even if the child is treated well. Those around it can kill it at any time and of course children don’t understand about laws against murder and so forth until much later in life.
It has been postulated that you can roughly determine the difference in strength between two people by taking the fourth power of the ratio of their heights.
Ref: [S. Gould. 1977. Ever Since Darwin. New York: W.W. Norton Company.]
The height of the average female is twice that of the average two year old so she is (24 = 16) sixteen times stronger than the child (2 to the power of 4). A very large difference in power and strength I think one could say. It has been postulated that around that age of 10 - 12 years is the first time where a child could probably start to look after itself in terms of acquiring the food and shelter necessary to live. Up until that time the child’s physical well being in terms of food and shelter is dependent on the adults around it. Of course the child knows that the adults can withdraw that food and shelter should they choose to do so.
Despite these physical threats we also have all the psychological causes of anxiety. If a child is psychologically abandoned in some way, which many are to varying degrees, anxiety is a common reaction to such abandonment. Children are much more psychologically dependent on those around them than adults are and thus anxiety may be more prevalent in childhood as a result.
Every parent also has a Child ego state of their own. Sooner or later there are going to be situations where their own Child ego state needs are going to take priority over the needs of their biological child. A classic example is post natal depression. In this case the mother’s own Child ego state needs may be to sleep for extended periods of time in bed as a consequence of the depression. When she does this her biological children’s psychological needs are secondary and thus anxiety can result when the children experience this psychological abandonment.
Finally normal human development requires the child to master scary developmental tasks. Most obviously the separations from mother and father. Such as going to school, handling difficult circumstances without mother’s help, getting a job and just becoming psychologically independent is an anxiety producing process.

There we have it. This could explain to some degree why childhood is more of an anxiety producing stage of human development as compared to adulthood. It does not seem possible to develop an argument for why childhood would be a more depression producing stage of development. Indeed the level of depression in childhood in the first piece of research cited put it at 21%. The statistics from the Department of health and ageing put the level of depression in adulthood at 20%. They are the same. Whereas anxiety in children seeking help was around 70% and in adulthood put around 10% of adults in general.
Nothing like a bit of hypothesising on a Friday!
Graffiti
Reported by school psychologists
Anxiety - 73.1%
Challenging behaviour - 71.8%
Family/parenting concerns - 65.4%
Peer relationships - 59%
Anger and conflict - 55.8%
Bullying - 41.7%
Self esteem - 38.5%
Child safety and protection - 31%
Depression - 21.1%
Trauma - 19.2%
Challenging behaviour = Autism spectrum disorder, ADHD, oppositional disorder, learning difficulties and conduct disorder
Ref: [Inpsych - Bulletin of the Australian Psychological Society, June 2011]
My work with children has mainly been in the private practice setting. Children are brought to me by their parents usually. The list cited above would be quite similar to how I would rate the children I have seen over the years.
One thing that has always interested me in my work with children, and what this data supports, is the low rate of depression as compared to the other mental health problems presented. I have found this surprising as I expected it to be higher. I expected anxiety to be as high as it is but I also expected depression to be the same. Which it is not. The rate of depression is much lower.
Why I expected this is because with adults and adolescents they tend to be about the same.
Adults in Australia (Department of health and ageing statistics)
10% anxiety at some point in adult life
20% depression (6% major depression)
One needs to be careful with such statistics as they can vary quite considerably depending on how one defines depression and anxiety. However, it seems safe to say that in adults there are similar amounts of depression compared to anxiety unlike in childhood. They are at similar rates whereas in childhood that is not the case with anxiety being much more prevalent than depression. According to the research above anxiety is three to four times more prevalent than depression in children seeking help from school psychologists.
This of courses raises the question as to why this would be so. I don’t know of any explanation that has been given to answer this question. So I thought I might do some hypothesising of my own.
Anxiety in childhood
It could be that diagnosing depression in children is harder than in adults. Thus the rates of depression are higher in children but are not recognised because the children do not present to school psychologists with that difficulty. I suppose this could be the case but it seems a bit dodgy to me as depression is not that hard to diagnose. Even if the child does not report the problem emotions found in depression the body language of a depressed child is not that hard to detect. It would also seem reasonable that a depressed child is just as likely to report unpleasant emotions as an anxious child. Why should there be any difference between those two?
It seems more reasonable to me that childhood by its very nature is more likely to produce reactions of anxiety rather than depression, whereas in adulthood this is not the case. It is simply a matter of when god made us, she stuffed up. The way humans reproduce the species is by giving birth to very small versions of adults that take almost two decades to fully mature.
As adults it is easy to forget just how vulnerable a child is. A child is like living in the land of the giants. Take a minute to lie face up on the floor, get someone to stand over you and remind yourself of how a child sees her relationships with adults.
One of my favourite TV shows in childhood - Land of the giants.
This could partly explain why anxiety is the highest of all mental health issues in childhood. A child’s life is on the line each day. Its actual physical existence is out of its control and is determined by those adults around her. Indeed a threatening state of affairs even if the child is treated well. Those around it can kill it at any time and of course children don’t understand about laws against murder and so forth until much later in life.
It has been postulated that you can roughly determine the difference in strength between two people by taking the fourth power of the ratio of their heights.
Ref: [S. Gould. 1977. Ever Since Darwin. New York: W.W. Norton Company.]
The height of the average female is twice that of the average two year old so she is (24 = 16) sixteen times stronger than the child (2 to the power of 4). A very large difference in power and strength I think one could say. It has been postulated that around that age of 10 - 12 years is the first time where a child could probably start to look after itself in terms of acquiring the food and shelter necessary to live. Up until that time the child’s physical well being in terms of food and shelter is dependent on the adults around it. Of course the child knows that the adults can withdraw that food and shelter should they choose to do so.
Despite these physical threats we also have all the psychological causes of anxiety. If a child is psychologically abandoned in some way, which many are to varying degrees, anxiety is a common reaction to such abandonment. Children are much more psychologically dependent on those around them than adults are and thus anxiety may be more prevalent in childhood as a result.
Every parent also has a Child ego state of their own. Sooner or later there are going to be situations where their own Child ego state needs are going to take priority over the needs of their biological child. A classic example is post natal depression. In this case the mother’s own Child ego state needs may be to sleep for extended periods of time in bed as a consequence of the depression. When she does this her biological children’s psychological needs are secondary and thus anxiety can result when the children experience this psychological abandonment.
Finally normal human development requires the child to master scary developmental tasks. Most obviously the separations from mother and father. Such as going to school, handling difficult circumstances without mother’s help, getting a job and just becoming psychologically independent is an anxiety producing process.
There we have it. This could explain to some degree why childhood is more of an anxiety producing stage of human development as compared to adulthood. It does not seem possible to develop an argument for why childhood would be a more depression producing stage of development. Indeed the level of depression in childhood in the first piece of research cited put it at 21%. The statistics from the Department of health and ageing put the level of depression in adulthood at 20%. They are the same. Whereas anxiety in children seeking help was around 70% and in adulthood put around 10% of adults in general.
Nothing like a bit of hypothesising on a Friday!
Graffiti
Monday, July 11, 2011
Book update - July
Working with suicidal individuals is now 6 months old. There have been three articles on it in the latest edition of WAVE magazine by journalist Milena Stosic.
A new review of the book found here.
An interview with me about my personal journey in the area as well as other questions about the book found here.
An article involving the psychological examination of three suicide notes - Adolf Hitler, Virginia Woolf and Sid Vicious of the Sex Pistols found here.
Order form for book can be found here.

The list of universities and colleges that now stock the book in their libraries for courses in psychology, counselling, social work and nursing continues to grow as well.
Maribor General Hospital Library (Slovenia)
Stellenbosch University Library (South Africa)
Mitt hogskolan library (Sweden)
Stockholm University (Sweden)
PJ Library (Norway)
University of Bergen (Norway)
Norges teknisk-naturvitenskapelige universitet (Norway)
University of Oslo (Norway)
University of Tromso (Norway)
University of Cambridge (UK)
Oxford University library (UK)
University of Exeter (UK)
Coventry City Council library (UK)
Bromley Library service (UK)
Cadbury Heath Library (UK)
Kingswood Library (UK)
Yate Library (UK)
British Library (UK)
Ebook library London (UK)
Hounslow Library (UK)
Barnet London Borough Library (UK)
National library of Scotland (Scotland)
Executive Counseling and Training Academy (Singapore)
Ngee Ann Polytechnic Library(Singapore)
Singapore Polytechnic Library (Singapore)
National University of Singapore (Singapore)
LaTrobe University (Aust)
Victoria University (Aust)
Queensland University of Technology (Aust)
Deakin University (Aust)
University of Western Australia (Aust)
University of Ballarat (Aust)
University of New England (Aust)
University of Western Sydney (Aust)
Charles Sturt University (Aust)
Curtin University (Aust)
Australian Catholic University (Aust)
University of Newcastle (Aust)
Bond University (Aust)
University of Melbourne (Aust)
James Cook University (Aust)
National Library of Australia (Aust)
University of California San Diego (USA)
Open Library. California State Library (USA)
Marquette University Raynor Memorial Library (USA)
University of Massachusetts Amherst (USA)
Williams College Massachusetts (USA)
National Library of Medicine Maryland (USA)
Illinois State University (USA)
Loyola Marymount University California (USA)
University of Michigan (USA)
Central Michigan University (USA)
University of North Carolina Chapel Hill (USA)
University of Missouri-Columbia (USA)
Akron-Summit County Public Library, Ohio (USA)
University of California Merced (USA)
University of North Carolina Greensboro (USA)
Library of congress (USA)
University of California San Franisco (USA)
Mt. Hood Community College Library Oregon (USA)
National College of Natural Medicine Oregon (USA)
Oregon Health and Science University (USA)
Northeast WI Public Libraries (USA)
College of DuPage Illinois (USA)
Boston College (USA)
University of Chicago Illinois (USA)
University of North Texas (USA)
Laredo Public Library Texas (USA)
University of Texas-Pan American (USA)
University of Texas at Austin (USA)
Trinity College Dublin (Ireland)
Dublin Institute of Technology (Ireland)
University of Auckland Library (New Zealand)
Auckland University of Technology (New Zealand)
Unitec Institute of Technology (New Zealand)
Eastern Institute of Technlogy (New Zealand)
University of Otago (New Zealand)
Rotorua District Library (New Zealand)
University of Waterloo (Canada)
Mount Royal University (Canada)
Wilfrid Laurier University (Canada)
University of Guelph (Canada)
Library and Archives Canada (Canada)
City University of Hong Kong (China)
Graffiti
A new review of the book found here.
An interview with me about my personal journey in the area as well as other questions about the book found here.
An article involving the psychological examination of three suicide notes - Adolf Hitler, Virginia Woolf and Sid Vicious of the Sex Pistols found here.
Order form for book can be found here.
The list of universities and colleges that now stock the book in their libraries for courses in psychology, counselling, social work and nursing continues to grow as well.
Maribor General Hospital Library (Slovenia)
Stellenbosch University Library (South Africa)
Mitt hogskolan library (Sweden)
Stockholm University (Sweden)
PJ Library (Norway)
University of Bergen (Norway)
Norges teknisk-naturvitenskapelige universitet (Norway)
University of Oslo (Norway)
University of Tromso (Norway)
University of Cambridge (UK)
Oxford University library (UK)
University of Exeter (UK)
Coventry City Council library (UK)
Bromley Library service (UK)
Cadbury Heath Library (UK)
Kingswood Library (UK)
Yate Library (UK)
British Library (UK)
Ebook library London (UK)
Hounslow Library (UK)
Barnet London Borough Library (UK)
National library of Scotland (Scotland)
Executive Counseling and Training Academy (Singapore)
Ngee Ann Polytechnic Library(Singapore)
Singapore Polytechnic Library (Singapore)
National University of Singapore (Singapore)
LaTrobe University (Aust)
Victoria University (Aust)
Queensland University of Technology (Aust)
Deakin University (Aust)
University of Western Australia (Aust)
University of Ballarat (Aust)
University of New England (Aust)
University of Western Sydney (Aust)
Charles Sturt University (Aust)
Curtin University (Aust)
Australian Catholic University (Aust)
University of Newcastle (Aust)
Bond University (Aust)
University of Melbourne (Aust)
James Cook University (Aust)
National Library of Australia (Aust)
University of California San Diego (USA)
Open Library. California State Library (USA)
Marquette University Raynor Memorial Library (USA)
University of Massachusetts Amherst (USA)
Williams College Massachusetts (USA)
National Library of Medicine Maryland (USA)
Illinois State University (USA)
Loyola Marymount University California (USA)
University of Michigan (USA)
Central Michigan University (USA)
University of North Carolina Chapel Hill (USA)
University of Missouri-Columbia (USA)
Akron-Summit County Public Library, Ohio (USA)
University of California Merced (USA)
University of North Carolina Greensboro (USA)
Library of congress (USA)
University of California San Franisco (USA)
Mt. Hood Community College Library Oregon (USA)
National College of Natural Medicine Oregon (USA)
Oregon Health and Science University (USA)
Northeast WI Public Libraries (USA)
College of DuPage Illinois (USA)
Boston College (USA)
University of Chicago Illinois (USA)
University of North Texas (USA)
Laredo Public Library Texas (USA)
University of Texas-Pan American (USA)
University of Texas at Austin (USA)
Trinity College Dublin (Ireland)
Dublin Institute of Technology (Ireland)
University of Auckland Library (New Zealand)
Auckland University of Technology (New Zealand)
Unitec Institute of Technology (New Zealand)
Eastern Institute of Technlogy (New Zealand)
University of Otago (New Zealand)
Rotorua District Library (New Zealand)
University of Waterloo (Canada)
Mount Royal University (Canada)
Wilfrid Laurier University (Canada)
University of Guelph (Canada)
Library and Archives Canada (Canada)
City University of Hong Kong (China)
Graffiti
Saturday, July 9, 2011
Anger and forgiveness in psychotherapy
On occasion there is the need for some anger expression in therapy. A recent example brought this to the fore.
A woman in her 50s had a life time of being ignored by her mother. But to make matters worse her two sisters were often highlighted by her mother at times in front of her. In public the mother may talk about the exploits and successes of her two sisters but never of her. It seems safe to say that there was favouritism in this way.
The woman would at times recount such situations that had occurred many times in her life and often felt anger as she did remember. When this happened it was not long until she would mention that she did not believe that her mother did this on purpose. That she was probably unaware that she was even doing such a thing. And from what I was told I tended to agree with her. In addition her mother was now quite elderly and frail and the client would say that how could she be angry at such an elderly person. Her goal was simply to forgive her mother for the mistreatment that she had received over the years in the way described above. However this meant she was directly avoiding being angry. Unfortunately this kept reappearing, her anger at her mother kept resurfacing.
As a therapist I am all in favour of the idea of forgiveness. I think it is a very wise psychological goal to aim for. Forgiving ones parents for that they did or forgiving ones abuser for the abuse received is a wise psychological goal. However sometimes this is the situation:
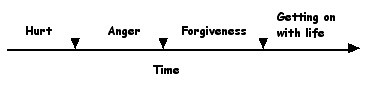
At times in order to get from the hurt to the forgiveness you have to go through a period of anger. If it is only a minor transgression then one does not have to. If it was significant especially at a young age and especially when over a period of time then one cannot go straight from the hurt to the forgiveness. They have to go through a period of anger.
This is where a lot of people get stuck, in one of two ways. Firstly, as in the case cited above the person is uncomfortable with anger and finds it difficult to go through that stage. They try all kinds of ways to avoid it and the example above shows some of the rationalisations that people will come up with in order to do that. Secondly, the other individual does not avoid it but gets stuck in it. This is not an uncommon scenario to come across in therapy. Some one who is chronically angry at their abuser. Quite often they never see their abuser now or the abuser may even be dead. The client may be carrying around a sack of anger on their back towards some one who died years ago. What does that achieve, and more importantly who suffers from the sack of anger - certainly not the dead person.

Some find forgiving their abuser this hard to do.
If the person does successfully transverse the anger then they are well on their way to achieving a sense of forgiveness. Once done, their life in the here and now is more pleasant and they are capable of more staisfying relationships in their current world. Indeed their current relationships are much less likely to be damaged by such unresolved past events.
However the difficult part for the therapist is to judge how long the angry period is meant to last. This is not an easy thing to gauge. As is often the case in therapy it is usually best to leave it up to the client and they will tell you in one way or another. However this is not always the case. For instance it is highly likely that the client described above will be saying she is ready to pass the angry stage before she is.

Living in the here and now. Can't enjoy this if your head is stuck in the past.
But she may tell the therapist in another way. Over time one will notice that she spontaneously brings up the issue of anger at mother less and less. When this happens she is ready to begin the forgiveness work and the therapist starts that phase of therapy.
Graffiti
A woman in her 50s had a life time of being ignored by her mother. But to make matters worse her two sisters were often highlighted by her mother at times in front of her. In public the mother may talk about the exploits and successes of her two sisters but never of her. It seems safe to say that there was favouritism in this way.
The woman would at times recount such situations that had occurred many times in her life and often felt anger as she did remember. When this happened it was not long until she would mention that she did not believe that her mother did this on purpose. That she was probably unaware that she was even doing such a thing. And from what I was told I tended to agree with her. In addition her mother was now quite elderly and frail and the client would say that how could she be angry at such an elderly person. Her goal was simply to forgive her mother for the mistreatment that she had received over the years in the way described above. However this meant she was directly avoiding being angry. Unfortunately this kept reappearing, her anger at her mother kept resurfacing.
As a therapist I am all in favour of the idea of forgiveness. I think it is a very wise psychological goal to aim for. Forgiving ones parents for that they did or forgiving ones abuser for the abuse received is a wise psychological goal. However sometimes this is the situation:
At times in order to get from the hurt to the forgiveness you have to go through a period of anger. If it is only a minor transgression then one does not have to. If it was significant especially at a young age and especially when over a period of time then one cannot go straight from the hurt to the forgiveness. They have to go through a period of anger.
This is where a lot of people get stuck, in one of two ways. Firstly, as in the case cited above the person is uncomfortable with anger and finds it difficult to go through that stage. They try all kinds of ways to avoid it and the example above shows some of the rationalisations that people will come up with in order to do that. Secondly, the other individual does not avoid it but gets stuck in it. This is not an uncommon scenario to come across in therapy. Some one who is chronically angry at their abuser. Quite often they never see their abuser now or the abuser may even be dead. The client may be carrying around a sack of anger on their back towards some one who died years ago. What does that achieve, and more importantly who suffers from the sack of anger - certainly not the dead person.
Some find forgiving their abuser this hard to do.
If the person does successfully transverse the anger then they are well on their way to achieving a sense of forgiveness. Once done, their life in the here and now is more pleasant and they are capable of more staisfying relationships in their current world. Indeed their current relationships are much less likely to be damaged by such unresolved past events.
However the difficult part for the therapist is to judge how long the angry period is meant to last. This is not an easy thing to gauge. As is often the case in therapy it is usually best to leave it up to the client and they will tell you in one way or another. However this is not always the case. For instance it is highly likely that the client described above will be saying she is ready to pass the angry stage before she is.
Living in the here and now. Can't enjoy this if your head is stuck in the past.
But she may tell the therapist in another way. Over time one will notice that she spontaneously brings up the issue of anger at mother less and less. When this happens she is ready to begin the forgiveness work and the therapist starts that phase of therapy.
Graffiti
Monday, July 4, 2011
Marriage counselling and the rise of individualism.
In Australia at the moment the number of people living single in a dwelling by them self is at a record high. There has never been a time when so many have lived single and not in a family unit or a group of some kind.
I have talked before about society, psychology and the rise of individualism.
I made mention that psychological theory over the past 150 years has promoted individualism as the psychologically healthy state. Since the contemplations of Freud, psychology has been very influential in directing governments to structure societies such that individualism thrives. To my mind this has gone too far and the individualism which psychological theory promotes has indeed become a neurotic condition itself.

This is no where better demonstrated than in marriage. The divorce rate in Australia hovers around the 50% mark and of those who don’t get divorced probably half of them would if they were not under pressure from religion, family and friends, financial pressure and so forth.
Anthropological studies show that as societies evolved originally you had to live in groups. People found that if you lived in a group your chances of survival were much better. This is no better demonstrated than in the basic family unit. When a male and a female produce a child, that child had a much better chance of survival if the mother and father stayed together.
Thus the psychology of these people one could postulate, was about the survival of the group rather than a focus on the ‘psychological survival’ of the individual. In addition to just survival people would have also discovered that if you lived in groups you could achieve things and create a much better lifestyle than if one simply existed on their own.
As societies mature and become more affluent then the basic survival needs become more predictable and guaranteed. People feel more secure about their basic survival. When this happens instead of feeling relief along comes Freud and the navel gazing starts. People start focussing on their own individual psychology and happiness. This now has progressed over generations of psychologists to the point where individualism is seen as the zenith to be achieved.
This change of focus from survival of the group to the pursuit of individual happiness is reflected of course in how therapists ply their trade, especially in marriage counselling. This quote comes from a psychology text book on marriage counselling that is used in universities and training institutes for psychologists.

If there was ever a need for a collectivist mindset for survival it is between comrades in a theatre of war.
“The client who, out of his own feeling of need, seeks marriage counselling obviously has some dissatisfactions with that relationship. Some of his needs are not being met, or for some reason his life pattern is not providing adequate satisfaction.”
Yikes!!!
out of his own feeling of need
some dissatisfactions with that relationship
some of his needs are not being met
Sometimes in couples counselling clients say to me, “This relationship is not meeting my needs.”
When I hear this I get a sort of flummoxed look on my face, and think:
Hello! Marriage is not a happy pill. Marriage is not this thing that is to meant make you feel better about yourself.
No wonder the divorce rate is what it is.
Individualism riding roughshod over the collective. And we are training our psychologists and marriage counsellors to espouse that very view to the public by putting such ideas in the very text books we use to train them.
My counselling of married couples has changed somewhat over the years. I was trained on those textbooks as well. My approach besides exposing the underlying dynamics of the relationship would promote behavioural negotiation between the couple such that both parties can get their needs met more comprehensively.

Now I do more along the lines of the acceptance of the other person for who they are. Not so much about getting my needs directly met by the other, more about accepting the other for who he/she is.
However I feel this is a superficial response to the shift away from individualism to a more collective approach in marriage counselling. I feel a more basic change is needed but I am not too sure what that is at the moment. It needs to involve more of a change in the philosophical outlook on marriage that can be woven into the therapeutic process.
Graffiti
I have talked before about society, psychology and the rise of individualism.
I made mention that psychological theory over the past 150 years has promoted individualism as the psychologically healthy state. Since the contemplations of Freud, psychology has been very influential in directing governments to structure societies such that individualism thrives. To my mind this has gone too far and the individualism which psychological theory promotes has indeed become a neurotic condition itself.
This is no where better demonstrated than in marriage. The divorce rate in Australia hovers around the 50% mark and of those who don’t get divorced probably half of them would if they were not under pressure from religion, family and friends, financial pressure and so forth.
Anthropological studies show that as societies evolved originally you had to live in groups. People found that if you lived in a group your chances of survival were much better. This is no better demonstrated than in the basic family unit. When a male and a female produce a child, that child had a much better chance of survival if the mother and father stayed together.
Thus the psychology of these people one could postulate, was about the survival of the group rather than a focus on the ‘psychological survival’ of the individual. In addition to just survival people would have also discovered that if you lived in groups you could achieve things and create a much better lifestyle than if one simply existed on their own.
As societies mature and become more affluent then the basic survival needs become more predictable and guaranteed. People feel more secure about their basic survival. When this happens instead of feeling relief along comes Freud and the navel gazing starts. People start focussing on their own individual psychology and happiness. This now has progressed over generations of psychologists to the point where individualism is seen as the zenith to be achieved.
This change of focus from survival of the group to the pursuit of individual happiness is reflected of course in how therapists ply their trade, especially in marriage counselling. This quote comes from a psychology text book on marriage counselling that is used in universities and training institutes for psychologists.
If there was ever a need for a collectivist mindset for survival it is between comrades in a theatre of war.
“The client who, out of his own feeling of need, seeks marriage counselling obviously has some dissatisfactions with that relationship. Some of his needs are not being met, or for some reason his life pattern is not providing adequate satisfaction.”
Yikes!!!
out of his own feeling of need
some dissatisfactions with that relationship
some of his needs are not being met
Sometimes in couples counselling clients say to me, “This relationship is not meeting my needs.”
When I hear this I get a sort of flummoxed look on my face, and think:
Hello! Marriage is not a happy pill. Marriage is not this thing that is to meant make you feel better about yourself.
No wonder the divorce rate is what it is.
Individualism riding roughshod over the collective. And we are training our psychologists and marriage counsellors to espouse that very view to the public by putting such ideas in the very text books we use to train them.
My counselling of married couples has changed somewhat over the years. I was trained on those textbooks as well. My approach besides exposing the underlying dynamics of the relationship would promote behavioural negotiation between the couple such that both parties can get their needs met more comprehensively.
Now I do more along the lines of the acceptance of the other person for who they are. Not so much about getting my needs directly met by the other, more about accepting the other for who he/she is.
However I feel this is a superficial response to the shift away from individualism to a more collective approach in marriage counselling. I feel a more basic change is needed but I am not too sure what that is at the moment. It needs to involve more of a change in the philosophical outlook on marriage that can be woven into the therapeutic process.
Graffiti
Sunday, July 3, 2011
Racket feelings
Emotions are such an emotive topic. There are many and varied definitions about them and lots of alternate theories of emotion. In transactional Analysis the term racket has been used in many ways and some are listed here.
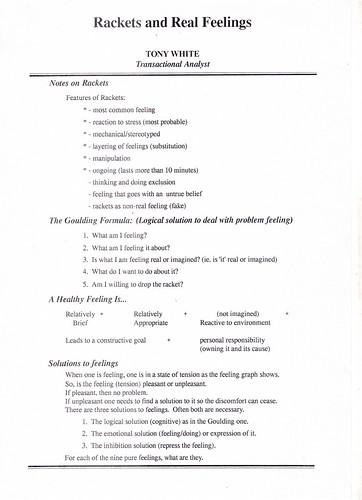
To see a larger version click on the picture.
Racket feelings are generally seen as pathological and hence it seems opportune to define what a healthy, here and now feeling is.
Also enclosed are different solutions to feelings. Again there is much conjecture on what is the psychologically healthy way to deal with feelings - express them, inhibit them or think them away.
Graffiti
To see a larger version click on the picture.
Racket feelings are generally seen as pathological and hence it seems opportune to define what a healthy, here and now feeling is.
Also enclosed are different solutions to feelings. Again there is much conjecture on what is the psychologically healthy way to deal with feelings - express them, inhibit them or think them away.
Graffiti
Saturday, July 2, 2011
Free Child communication in relationships
As a marriage or couples counsellor a common problem one sees is about the Free Child in relationships. In terms of the perceived quality of a relationship or a relationship that is wanted by both parties then these types of transactions must occur at least some of the time.
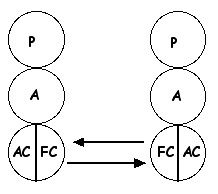
To understand such a diagram just think of a relationship which you like and enjoy and have a desire to be involved in. It is highly likely you have just identified a relationship in your life that has a significant amount of Free Child transactions between you and the other party.
In the honeymoon stage of a relationship these types of transactions occur quite often. Of course a solid relationship involves much more than just FC to FC transactions but my point here is that if a relationship does not have such communication then it will tend to fall on hard times. If there is very little then the ‘end is nigh’ often.
As a marriage counsellor one often sees couples who present with this type of communication problem, few FC transactions. This often occurs because the Free Child of both parties have ‘left the building’ as they say. The sensitive part of the personality has retreated into hiding for some reason.
Elvis leaving the building
In particular there are two common scenarios where this happens and presents a very real and difficult situation for the couple. This is often presented in marriage counselling and guess what they both involve sex and drugs! Why you may ask, because both sex and drugs often involve a degree of Free Child if not lots of Free Child.
Sex
Level of libido of a couple. If the couple have these combinations then sex is not going to be so much of a problem or at least it is a very good start for the couple not having difficulties in their sexual relationship. Both parties are either:
Low & low
Medium & medium
High & high
If they are either
Low & medium
Medium & high
then there is the potential for some degree of problem. If they are
Low & high
then there is a very real possibility of difficulties.

Why is this so? Because the Free Child is going to be affected. If the male has a high libido and the female has a low libido (which is usually the combination) then they have a significant problem that could contribute to destroying the relationship.
He is going to be asking for sexual contact often (or at least feel the desire to ask often). She is going to want much less. If she says yes when she wants to say no, it wont be long before her FC starts to retreat into the distance. She is having intimate physical sexual contact when she does not want it and the FC is not going to tolerate that for very long at all.
If she says no when she wants to say no (which will be often due to the different levels of libido) then one problem is solved but another is created. Her FC will feel satisfied but his wont be. His FC will feel ‘ripped off’ in some way. If this is occasional it does not matter all that much. But if it is happening most days what will happen after 5, 10 or 15 years? His FC is going to have disappeared in a similar fashion long ago.
A very real and difficult problem for a couple.

Cooperation in the relational
Alcohol and drugs
The most common scenario is the male likes a drink or a smoke and the wife finds him unpleasant or repugnant when he is intoxicated. The wife may say things like:
“He is embarrassing when he has been drinking”
“He snores loudly when he has been drinking”
“It is bad for the kids to see him like that”
“He may drive while intoxicated”
and so forth
So she asks, demands, threatens that he does not drink or use drugs (or significantly reduces the use). If he obliges and stops then her FC needs are met but this creates another problem. His FC will feel ‘ripped off’ in some way. If he continues to drink then his FC needs are meet but her FC will retreat into the distance.
After this occurring for 10 years what is likely to happen? Either one or both FC ego states have disappeared out of the relationship and probably do not even want to come back.
A very real and difficult problem for a couple.
In both these instances there are no winners. No matter which solution you take both parties loose in the long run.
It is best if the couple do not allow it to become such a large issue in the relationship. That’s easy for a bystander to say when not directly involved in it. Also most couples do not realise it is becoming a big issue until it gets there. And as I have said before most couples actually get into couples counselling 6 to 12 months late when the small issues have evolved into the very communication style of the couple. It is best to get to the problem when it is still relationship dystonic not when it has evolved into a relationship syntonic problem.
Graffiti
To understand such a diagram just think of a relationship which you like and enjoy and have a desire to be involved in. It is highly likely you have just identified a relationship in your life that has a significant amount of Free Child transactions between you and the other party.
In the honeymoon stage of a relationship these types of transactions occur quite often. Of course a solid relationship involves much more than just FC to FC transactions but my point here is that if a relationship does not have such communication then it will tend to fall on hard times. If there is very little then the ‘end is nigh’ often.
As a marriage counsellor one often sees couples who present with this type of communication problem, few FC transactions. This often occurs because the Free Child of both parties have ‘left the building’ as they say. The sensitive part of the personality has retreated into hiding for some reason.
Elvis leaving the building
In particular there are two common scenarios where this happens and presents a very real and difficult situation for the couple. This is often presented in marriage counselling and guess what they both involve sex and drugs! Why you may ask, because both sex and drugs often involve a degree of Free Child if not lots of Free Child.
Sex
Level of libido of a couple. If the couple have these combinations then sex is not going to be so much of a problem or at least it is a very good start for the couple not having difficulties in their sexual relationship. Both parties are either:
Low & low
Medium & medium
High & high
If they are either
Low & medium
Medium & high
then there is the potential for some degree of problem. If they are
Low & high
then there is a very real possibility of difficulties.
Why is this so? Because the Free Child is going to be affected. If the male has a high libido and the female has a low libido (which is usually the combination) then they have a significant problem that could contribute to destroying the relationship.
He is going to be asking for sexual contact often (or at least feel the desire to ask often). She is going to want much less. If she says yes when she wants to say no, it wont be long before her FC starts to retreat into the distance. She is having intimate physical sexual contact when she does not want it and the FC is not going to tolerate that for very long at all.
If she says no when she wants to say no (which will be often due to the different levels of libido) then one problem is solved but another is created. Her FC will feel satisfied but his wont be. His FC will feel ‘ripped off’ in some way. If this is occasional it does not matter all that much. But if it is happening most days what will happen after 5, 10 or 15 years? His FC is going to have disappeared in a similar fashion long ago.
A very real and difficult problem for a couple.
Cooperation in the relational
Alcohol and drugs
The most common scenario is the male likes a drink or a smoke and the wife finds him unpleasant or repugnant when he is intoxicated. The wife may say things like:
“He is embarrassing when he has been drinking”
“He snores loudly when he has been drinking”
“It is bad for the kids to see him like that”
“He may drive while intoxicated”
and so forth
So she asks, demands, threatens that he does not drink or use drugs (or significantly reduces the use). If he obliges and stops then her FC needs are met but this creates another problem. His FC will feel ‘ripped off’ in some way. If he continues to drink then his FC needs are meet but her FC will retreat into the distance.
After this occurring for 10 years what is likely to happen? Either one or both FC ego states have disappeared out of the relationship and probably do not even want to come back.
A very real and difficult problem for a couple.
In both these instances there are no winners. No matter which solution you take both parties loose in the long run.
It is best if the couple do not allow it to become such a large issue in the relationship. That’s easy for a bystander to say when not directly involved in it. Also most couples do not realise it is becoming a big issue until it gets there. And as I have said before most couples actually get into couples counselling 6 to 12 months late when the small issues have evolved into the very communication style of the couple. It is best to get to the problem when it is still relationship dystonic not when it has evolved into a relationship syntonic problem.
Graffiti
Subscribe to:
Posts (Atom)