Tony White
7 July, 2007
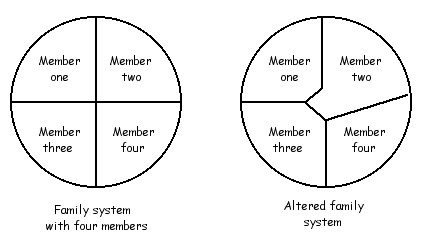
Weight loss is always a Parent ego state contract.
When someone seeks counselling to loose weight one can be fairly safe in saying
that it will be a Parent contract at least in part. A Parent contract is a
contract for change made from the Parent ego state. Contracts from the Parent
ego state rarely work, or they can work for a little while and then don't.
For example a contract (or goal) to loose weight, or to stop drinking, or to
exercise more, or to stop taking drugs, or to work harder are all Parent
contracts to some extent. The reason why they don't last is because they involve
deprivation of the Child ego state, namely the Free Child. When people (the Free
Child) discover something feels good then there is quire a strong drive to have
more of it. This seems to be the normal human condition. If someone discovers
that they very much like the taste of fish and chips then there will be quite a
strong urge to have such food more often.
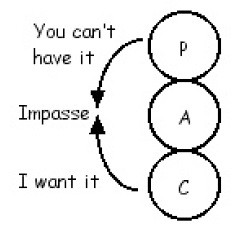
In reaction to this FC urge the person's Parent ego state may then say "no you
cannot eat fish and chips because they make you fat and are unhealthy". When
this happens then one has intrapsychic conflict. This means there is a conflict
between two parts of the psyche. In this case the Free Child and the Parent ego
state are in conflict. They are at an impasse.
The originator of Gestalt therapy (Fritz Perls) used to talk about it and called it
a battle between top dog and bottom dog. In Transactional Analysis the conflict
is between the Parent and the Child ego states. In the final analysis it is the
bottom dog that wins, or it is the Child that wins out in some way.
It look like Free Child
This raises the question; What happens if FC does not get its needs met? A
number of factors come into play at this point. The first is the degree of the
deprivation. If one is deprived of food the need is very high. If one is deprived
of their favourite TV show for a week then the need may not be so high. Also it
depends on the amount of frustration tolerance the person has.
If a teenager is told they can't go out one Saturday night, some will take it on
the chin whereas others who tolerate frustration much less well may provide
quite a dramatic response.
Some one used to say, "People are where they want to be". Another way of saying
this is, "where there is a will there is a way". Sooner or later the Child ego state
will get its way. So sooner or later the deprived person will get their fish and
chips. When the Parent ego state says no because you will get fat, sooner or
later the Child will get the food in some form. Hence there is no weight lost and
usually there is some put on!

However some people do loose weight. I once saw a journal article titled, "The
anti-diet approach to weight loss". This approach works for those people who
harass themselves. They get strokes by putting themselves down. Those who have
a large internal Critical Parent ego state. If they give them self permission to
eat what they want (anti-diet) then they are more likely to loose weight.
In this instance the person eats and then criticises self for eating and putting
on weight. In this type of weight gain it is the after effect (or hangover) that is
important. So if the person allows self to eat anything they want and not
criticise self then the psychological purpose for the poor eating ceases. Then the
person will tend to eat in a more healthy fashion.
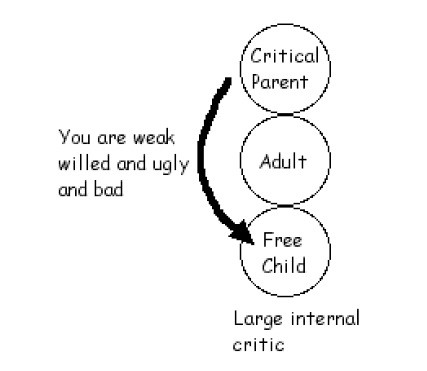
The game of “Internal critic” results in lots of negative strokes or
reinforcement of the eating behaviour
What have I done here?. I have refused to address the weight loss directly (ie
not taken the Parent contract) and snuck around the side and gone through that
door. How?
1. I have discovered the psychological function that the eating/weight gain
serves. It is a source of strokes and results in the game of "internal critic".
2. I have gotten rid of that function (ie the negative stroking and the game)
3. Thus the negative strokes and the game serve no psychological function any
more and thus using eating to get such strokes ceases.
Of course there are other reasons why people over eat and carry excessive
weight but this is just one example of how one can avoid the Parent contract
that a weight loss contract always is.
The psychology of food
With all the comment around about obesity in society, I thought I would make
some comments on the psychology of food and eating that I have seen over the
years.
Food and strokes.
As we know we all need psychological strokes(Attention) to survive and remain
sane. Without them we quickly deteriorate as happens to someone when they are
put into solitary confinement. Food is a very rich and good supply of positive
strokes. Food feels good and not only does one get the strokes from food but the
strokes are physical and inside our very bodies. Food can make us feel good inside.
Very few other things can do that besides alcohol and drugs.
So if someone is stroke deprived then they can become an over eater as it
becomes one of their main sources of strokes. The good part about this is that it
is relatively easy to alter. If the person starts to develop other stroke sources
then the food intake can decrease as it looses some of its psychological
importance.
As food is a strong positive stroke, if someone is in an environment where they
are getting many negative strokes it is appealing to eat as it is one way in which
they can get positive strokes. Sometimes this is called 'comfort eating'. The
strokes from the eating makes one feel 'comforted' and pampered. If one lives
around people who are quite critical environment one can understand why some
eat for comfort.
(A harsh environment can lead to comfort eating to make it feel a bit better, and
it does).
Sometimes the 'harsh' environment can even be inside the persons own head. If
someone has been traumatised by some event in their life then they can feel
considerable pain, angst, anxiety and so on, over and over in their own head.
"Comfort" eating can help ease some of that internal pain. The problem is the
person eats to satiate hunger AND eats to get comfort and that usually results
in over eating.
As we know kids copy parents and if parents are critical of them in childhood
then they internalise that critical parent in their own head. Thus in later life
they can have a big internal critic that jumps on them given the slightest
opportunity. Again comfort eating can be used as a counter to this large internal
critic that one has in side their own head.

(Humans sometimes cannot even recognize when they have enough food)
If the issue of power is poorly handled by parents then a power struggle can
develop between child and parent. This power struggle can be lived out in a
variety of formats such as through temper tantrums or being disobedient. It can
also be lived out through eating. All parents want children to eat and to eat
healthy food. Children learn this and can fight with parents by not eating or not
eating properly. This is a very common feature in anorexia where the child can be
claiming its own sense of personal power by not eating. The same can happen the
other way where the person can defy the parents by over eating.
This can also manifest in another way where the person has a sense of loosing
their own power with themselves. Those with eating disorders often report that
their eating is out of control, many obese people feel like this at least from time
to time. “I have a sense of disempowerment and thus my eating is out of control”.
Food and sex
How one looks physically is determined to a large extent by how much one eats.
Sex involves two people being physically very close and thus both parties see the
other persons body to some degree. In this way over eating and thus obesity can
be used as a protection against sex.
"If I am fat, therefore I am ugly and thus no one will want to have sex with me".
"I just feel so bad about how I look I can't have my husband see or touch me and
thus we can't have sex"
These are two views that some women and men to a lesser degree can maintain.
The psychological drive behind it is a fear of sex, or some other emotional
problem with sex.
Food and feelings
This one is a huge area which can result in over eating. Food and feelings get
mixed up in some way. Sometimes food and love get mixed up. Mother’s sometimes
find that they can express love to their children by feeding them. This is
particularly so if the mother has difficulty with the more open and direct
expression of love and closeness to a child. So she feeds him up instead and that
is how she shows her love to the child
But it does not end there. It does not take long for the child to realise this and
then the mother can use guilt. “If you don’t eat all your food then you are
rejecting me and then I feel bad”, can be the mother’s attitude. Thus the child
will feel guilty if it does not eat the food mother prepares. This will usually
result in over eating to some degree.
Food can be used as a way of dealing with a child’s emotions and emotional
distress. If a child gets angry the mother may think, “That must mean he is
hungry” and she gives him a sandwich. The child starts to mix up anger and hunger
and that can easily lead to obesity. In adulthood every time the person gets
angry they eat. If a child gets distressed about finding his goldfish dead mother
maybe at a loss of how to deal with the distress so she gives him a freshly baked
muffin. Distress and hunger get mixed up and that person later in life solves
their own distress by eating.
As is so often the case, physical activities that are crucial to our physical
survival, such as eating, easily become encased in a web of psychology for the
person. They cease to remain a simple biological function and get embroiled in
powerful psychological motives.
Self esteem
In each of us we all have our ideal or perfect self and our real or actual self.
IDEAL or PERFECT self
Our ideal self is they way we would like to be. How much we should weigh, how our
hair should be, how popular we are meant to be, how funny we are supposed to be,
how we want our nose to be and so on for many, many things.
REAL or ACTUAL self
This is the way we actually see ourselves. How popular we actually think we are,
how our hair actually is, how much we actually weigh, how funny we actually think
we are and so on.
In everybody the IDEAL self is always above the REAL self. Everyone wants to
be different in some ways. Everyone wants to have a bit more of this or a bit
less of that in our bodies and our personalities. It is a matter of degree. For
some people the difference between the IDEAL self and the REAL self is small.
When this is so these people will have a good self esteem. They like themselves.
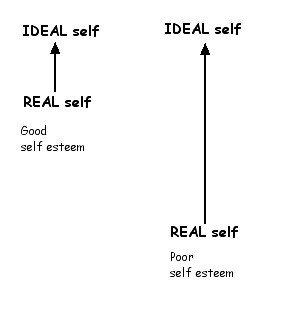
For other people the difference between the IDEAL self and the REAL self is
very big. How they actually are is very much below what they see as being ideal
or perfect. These people will have a poor self esteem. They do not think much of
themselves. They do not like themselves.

The ideal me
To get the IDEAL self and the REAL self closer it is much easier and better to
make the IDEAL self lower rather than the REAL self higher.
Instead of thinking the IDEAL self is 45 kg it can be 55 kg
Instead of thinking that you have to have a nose like Nicole Kidman you think
that other types of noses are OK as well
Instead of thinking that you have to be like the most popular girl in the class you
think that you can be more how you are.
If you do things like this then you will feel better about yourself and you will
have a better self esteem.