This is a follow on from the post before on human attachment.
Sometimes however children do not go through the attachment build up followed by the attachment breakdown. Consider the experiments done by John Bowlby with attachment many years ago.
A mother and young child would go into a room that had a chair in the middle. In the room there would be toys and other interesting things for a child to look at and play with. The mother sits in the chair by herself or just talks with another adult. The researchers then simply observed what the child did and there were three patterns that came up.

1. Some children would stay next to mother but slowly and surely move away from her to investigate the room. They would move away and then come back and then move away again further and further each time. Checking on mother from time to time. This they called a secure attachment
2. Some children just moved away from mother did not look back at her or seek her out again and amused themselves with the toys. This is called an isolated attachment as the child did not use mother as a secure home base. Typical in later life of the schizoid personality
3. Some children never left mother’s side . They may look around the room at the interesting stuff but never left mother’s side in any significant way. This is called an insecure attachment. This is the psychological basis of the addictive personality. They never adequately learnt the process of the attachment breakdown.

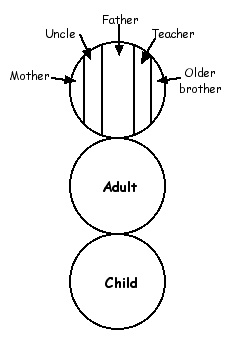
The vast majority of children learn how to form an attachment. Those who don’t end up showing autistic like symptoms. Children will develop an attachment to a parent who treats them well and also to the parent who treats them badly. The need to form an attachment is that essential for the psychological well being of the child. The stockholm syndrome is an example of those who developed an attachment to their abuser as do young children.
However the process of breaking down the attachment is not learnt by all, those who don’t can develop the insecure attachment and continually seek mother’s side. As we know the essential feature of an attachment is the desire to maintain proximity with the attachment figure. Thus the child’s reluctance to leave mother’s proximity.

The dependent personality is the same and this explains the ‘drug addict’ type of drug user. These are the ones who find it really, really, really hard to stop using. People use drugs for many reasons and these are the ones often portrayed in the movies, usually live wretched lives and use up most of the health, legal and counselling resources in the community. In number they are quite small but they use up most of the resources allocated to drug users in the community because drugs ruin their lives, families and often they are outside the law and require health resources as a result of their drug taking. Listening to these people talk about the drug one finds an uncanny similarity to talking about a relationship with a husband or wife. The drug becomes their partner.
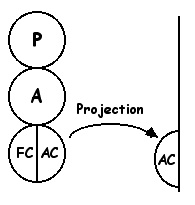
As they grow through life into adulthood they discover something that feels good for them. That can be anything with the most common ones being cigarettes, alcohol, drugs, food, sex, gambling, religion, another person and they in essence form an attachment to it. As they never developed the ability to break the attachment down they then form an insecure attachment with the ‘thing’. Thus they have a continual heightened desire to maintain proximity with it and thus one ends up with the addiction. It is an attachment problem.
In the histories of drug addicts one finds they have gotten off the drugs on many occasions. Their problem is not to get off the drug but to stay off the drug. When they remove self from the attachment figure (drug) they find it so difficult to maintain the distance that they they sooner or later again seek the proximity of the attachment figure and thus start using again.
Graffiti