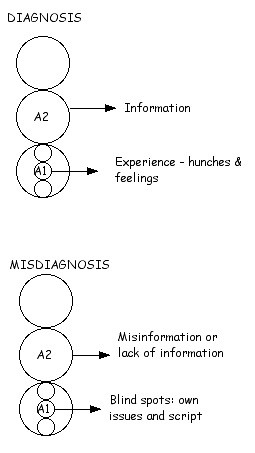
This diagram shows how therapists make diagnoses of the client. It is a function of the Adult ego state (A2) and the Little Professor ego state (A1).
Therapists are making diagnostic conclusions all the time. This can be formal diagnoses such as OCD, PND, DID, PD, ADD. (that is an awful lot of Ds) or all sorts of little diagnostic conclusions in each therapy session. What the body language may be saying, the client maybe seen as minimising, rationalising, displaying racket feelings and so on many, many times each session.
It seems safe to say that all therapists will believe things about clients that are not true. Most often they are things which are not of any great significance. Occasionally they are and then there is a problem.
Over the years I have received referral notes from a whole variety of different professionals. At times the referral note includes a diagnosis of the client being referred. After getting to know the client a bit I sometimes find my diagnosis is different to the referrer. We both can’t be right.

What is the diagnosis?
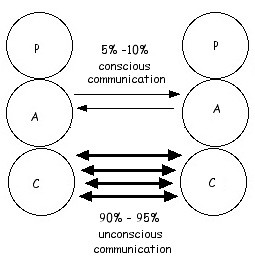
Diagnosis involves receiving Adult information and then making conclusions based on that. However as this diagram shows humans receive a huge amount of information unconsciously. In Transactional Analysis terms this information is processed by the little adult of the Child ego state (sometimes referred to as the Little Professor ego state). If therapists use this in their diagnosis then they are using hunches and feelings to decide on the diagnosis.
At the Adult ego state level misdiagnosis can occur because there is misinformation, a lack of information or the therapist is mistaken about what the information means.
Diagnosis with the A1 unconscious information is a double edged sword. It can result in more swift and insightful diagnoses but it also has the potential to go more awry than an A2 diagnosis.
Each of us also have our blind spots - our own personal issues and script. Some people see sexual abuse every where, if one has personal issues about the opposite sex then diagnosis in couples counselling can be way off, people who lack a sense of trust themselves will tend to see trust issues more often in their clients, or alternatively they may miss an obvious diagnosis of trust issues.
Another cause of misdiagnosis is inter-professional rivalry - “My theory is bigger and better than your theory”. In some circumstances there is considerable money, power and prestige invested in making certain diagnoses and particularly believing in a particular aetiology for the diagnosis. One needs to be careful that their Child ego state does not take over here and the client suffers or becomes secondary to proving ones diagnosis for professional pride. A diagnosis must always remain changeable in the mind of the diagnostician, when one resists such a change it is necessary to look at ones real motives.

Unruly child = ADD?
Psychology is subject to fashion and trends like any other area of human endeavour. There will be fashions in diagnosis as well. An example of this is ADD. Once upon a time ADD was a discrete and identifiable diagnostic condition. In recent years in Australia it has become a very fashionable diagnosis and now any unruly child can be diagnosed with ADD. Another example of this is the diagnosis of drug induced psychosis. This is a very politically correct and fashionable diagnosis in Australia at this time. Hence it is over diagnosed and thus the therapist believes something about the client which is untrue.
Graffiti
thanks, really nice article!
ReplyDelete